Evan Czulada, Rajiv Kabadi, Binaya Basyal, Cyrus Hadadi, Athanasios Thomaides
{"title":"具有挑战性的提取和更换一个8年的纳米刺激无铅起搏器和AVEIR植入物。","authors":"Evan Czulada, Rajiv Kabadi, Binaya Basyal, Cyrus Hadadi, Athanasios Thomaides","doi":"10.19102/icrm.2024.15126","DOIUrl":null,"url":null,"abstract":"<p><p>Leadless pacemakers (LPs) are emerging options for bradyarrhythmias. However, extraction can be risky if the device is in an unfavorable position. We present a challenging case of a Nanostim LP (NLP) (Abbott Medical Inc., Abbott Park, IL, USA) placed 8 years prior to removal and subsequent replacement with an AVEIR LP (ALP) (Abbott). A 72-year-old man received an NLP in 2015 for persistent atrial fibrillation with bradycardia. The NLP could not be interrogated in our office. An external event monitor demonstrated persistent atrial fibrillation with bradycardia and pauses. A premature battery depletion of the NLP was suspected. An ALP was chosen for replacement. On a computed tomography scan of the chest, the NLP was seen in the mid-free wall of the right ventricle, and its proximal portion abutted the tricuspid annulus. The AVEIR retrieval catheter (ARC) was used for retrieval. Multiple attempts were made to snare the device, yet it proved difficult due to poor placement and button tissue formation. The snare became damaged, and a second ARC was needed. On the successful attempt, the NLP was snared proximally and permitted docking. We advanced the protective sleeve over the NLP body, but resistance was observed due to tissue growth. Counterclockwise torsion was applied, and the device disconnected. Once the NLP was in linear orientation, the protective sleeve was eventually positioned over its body, allowing removal. The ALP was then installed without difficulty or structural complications. This report shows the importance of proper LP placement in the right ventricular septal wall. LP removal can be performed safely, yet complications can arise based on the age and location of the LP. The ARC can be successfully used to extract non-AVEIR LPs with evidence of docking button tissue growth. Similar interventions should exercise caution when attempting extraction and subsequent implantation.</p>","PeriodicalId":36299,"journal":{"name":"Journal of Innovations in Cardiac Rhythm Management","volume":"15 12","pages":"6126-6129"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11717154/pdf/","citationCount":"0","resultStr":"{\"title\":\"Challenging Extraction and Replacement of an Eight-year-old Nanostim Leadless Pacemaker and AVEIR Implant.\",\"authors\":\"Evan Czulada, Rajiv Kabadi, Binaya Basyal, Cyrus Hadadi, Athanasios Thomaides\",\"doi\":\"10.19102/icrm.2024.15126\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Leadless pacemakers (LPs) are emerging options for bradyarrhythmias. However, extraction can be risky if the device is in an unfavorable position. We present a challenging case of a Nanostim LP (NLP) (Abbott Medical Inc., Abbott Park, IL, USA) placed 8 years prior to removal and subsequent replacement with an AVEIR LP (ALP) (Abbott). A 72-year-old man received an NLP in 2015 for persistent atrial fibrillation with bradycardia. The NLP could not be interrogated in our office. An external event monitor demonstrated persistent atrial fibrillation with bradycardia and pauses. A premature battery depletion of the NLP was suspected. An ALP was chosen for replacement. On a computed tomography scan of the chest, the NLP was seen in the mid-free wall of the right ventricle, and its proximal portion abutted the tricuspid annulus. The AVEIR retrieval catheter (ARC) was used for retrieval. Multiple attempts were made to snare the device, yet it proved difficult due to poor placement and button tissue formation. The snare became damaged, and a second ARC was needed. On the successful attempt, the NLP was snared proximally and permitted docking. We advanced the protective sleeve over the NLP body, but resistance was observed due to tissue growth. Counterclockwise torsion was applied, and the device disconnected. Once the NLP was in linear orientation, the protective sleeve was eventually positioned over its body, allowing removal. The ALP was then installed without difficulty or structural complications. This report shows the importance of proper LP placement in the right ventricular septal wall. LP removal can be performed safely, yet complications can arise based on the age and location of the LP. The ARC can be successfully used to extract non-AVEIR LPs with evidence of docking button tissue growth. Similar interventions should exercise caution when attempting extraction and subsequent implantation.</p>\",\"PeriodicalId\":36299,\"journal\":{\"name\":\"Journal of Innovations in Cardiac Rhythm Management\",\"volume\":\"15 12\",\"pages\":\"6126-6129\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-12-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11717154/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Innovations in Cardiac Rhythm Management\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.19102/icrm.2024.15126\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Innovations in Cardiac Rhythm Management","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.19102/icrm.2024.15126","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Challenging Extraction and Replacement of an Eight-year-old Nanostim Leadless Pacemaker and AVEIR Implant.
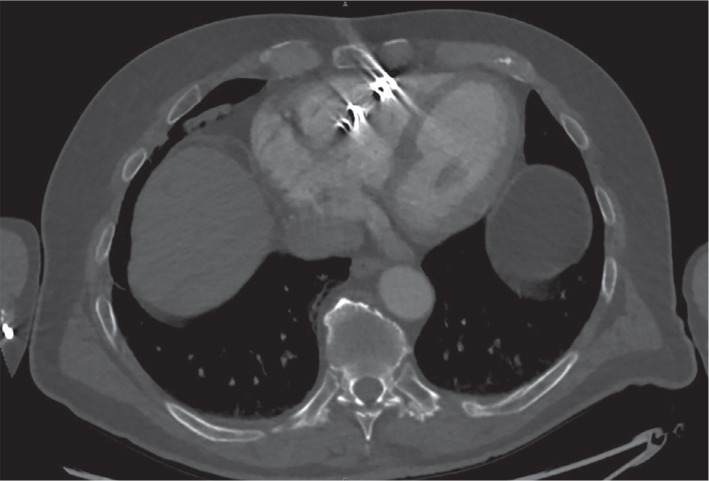
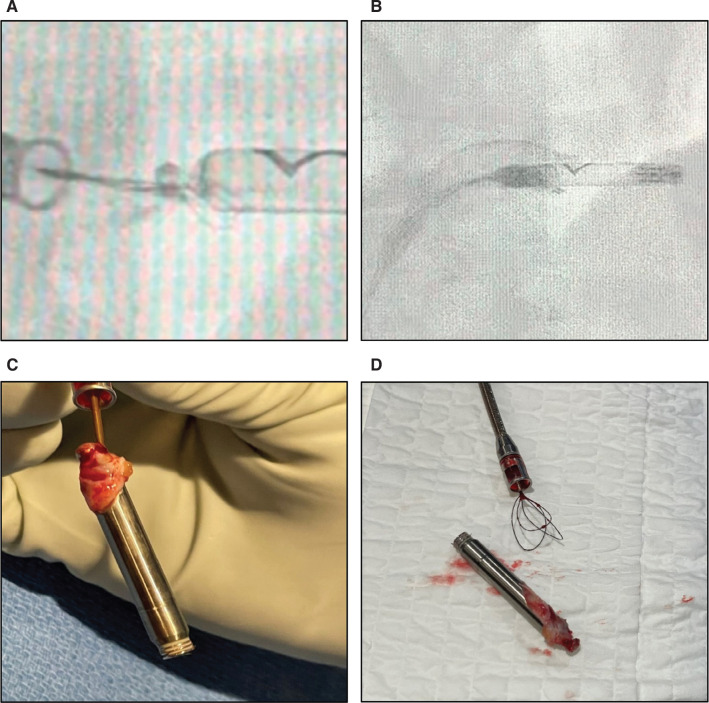
Leadless pacemakers (LPs) are emerging options for bradyarrhythmias. However, extraction can be risky if the device is in an unfavorable position. We present a challenging case of a Nanostim LP (NLP) (Abbott Medical Inc., Abbott Park, IL, USA) placed 8 years prior to removal and subsequent replacement with an AVEIR LP (ALP) (Abbott). A 72-year-old man received an NLP in 2015 for persistent atrial fibrillation with bradycardia. The NLP could not be interrogated in our office. An external event monitor demonstrated persistent atrial fibrillation with bradycardia and pauses. A premature battery depletion of the NLP was suspected. An ALP was chosen for replacement. On a computed tomography scan of the chest, the NLP was seen in the mid-free wall of the right ventricle, and its proximal portion abutted the tricuspid annulus. The AVEIR retrieval catheter (ARC) was used for retrieval. Multiple attempts were made to snare the device, yet it proved difficult due to poor placement and button tissue formation. The snare became damaged, and a second ARC was needed. On the successful attempt, the NLP was snared proximally and permitted docking. We advanced the protective sleeve over the NLP body, but resistance was observed due to tissue growth. Counterclockwise torsion was applied, and the device disconnected. Once the NLP was in linear orientation, the protective sleeve was eventually positioned over its body, allowing removal. The ALP was then installed without difficulty or structural complications. This report shows the importance of proper LP placement in the right ventricular septal wall. LP removal can be performed safely, yet complications can arise based on the age and location of the LP. The ARC can be successfully used to extract non-AVEIR LPs with evidence of docking button tissue growth. Similar interventions should exercise caution when attempting extraction and subsequent implantation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


