Zyad James Carr, Daniel Agarkov, Judy Li, Jean Charchaflieh, Andres Brenes-Bastos, Jonah Freund, Jill Zafar, Robert B Schonberger, Paul Heerdt
{"title":"在大容量术前评估诊所实施简短的亚极限心肺测试:可行性研究。","authors":"Zyad James Carr, Daniel Agarkov, Judy Li, Jean Charchaflieh, Andres Brenes-Bastos, Jonah Freund, Jill Zafar, Robert B Schonberger, Paul Heerdt","doi":"10.2196/65805","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Precise functional capacity assessment is a critical component for preoperative risk stratification. Brief submaximal cardiopulmonary exercise testing (smCPET) has shown diagnostic utility in various cardiopulmonary conditions.</p><p><strong>Objective: </strong>This study aims to determine if smCPET could be implemented in a high-volume presurgical evaluation clinic and, when compared to structured functional capacity surveys, if smCPET could better discriminate low functional capacity (≤4.6 metabolic equivalents [METs]).</p><p><strong>Methods: </strong>After institutional approval, 43 participants presenting for noncardiac surgery who met the following inclusion criteria were enrolled: aged 60 years and older, a Revised Cardiac Risk Index of ≤2, and self-reported METs of ≥4.6 (self-endorsed ability to climb 2 flights of stairs). Subjective METs assessments, Duke Activity Status Index (DASI) surveys, and a 6-minute smCPET trial were conducted. The primary end points were (1) operational efficiency, based on the time of the experimental session being ≤20 minutes; (2) modified Borg survey of perceived exertion, with a score of ≤7 indicating no more than moderate exertion; (3) high participant satisfaction with smCPET task execution, represented as a score of ≥8 (out of 10); and (4) high participant satisfaction with smCPET scheduling, represented as a score of ≥8 (out of 10). Student's t test was used to determine the significance of the secondary end points. Correlation between comparable structured surveys and smCPET measurements was assessed using the Pearson correlation coefficient. A Bland-Altman analysis was used to assess agreement between the methods.</p><p><strong>Results: </strong>The mean session time was 16.9 (SD 6.8) minutes. The mean posttest modified Borg survey score was 5.35 (SD 1.8). The median patient satisfaction (on a scale of 1=worst to 10=best) was 10 (IQR 10-10) for scheduling and 10 (IQR 9-10) for task execution. Subjective METs were higher when compared to smCPET equivalents (extrapolated peak METs; mean 7.6, SD 2.0 vs mean 6.7, SD 1.8; t<sub>42</sub>=2.1; P<.001). DASI-estimated peak METs were higher when compared to smCPET peak METs (mean 8.8, SD 1.2 vs mean 6.7, SD 1.8; t<sub>42</sub>=7.2; P<.001). DASI-estimated peak oxygen uptake was higher than smCPET peak oxygen uptake (mean 30.9, SD 4.3 mL kg<sup>-1</sup> min<sup>-1</sup> vs mean 23.6, SD 6.5 mL kg<sup>-1</sup> min<sup>-1</sup>; t<sub>42</sub>=7.2; P<.001).</p><p><strong>Conclusions: </strong>Implementation of smCPET in a presurgical evaluation clinic is both patient centered and clinically feasible. Brief smCPET measures, supportive of published reports regarding low sensitivity of provider-driven or structured survey measures for low functional capacity, were lower than those from structured surveys. Future studies will analyze the prediction of perioperative complications and cost-effectiveness.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT05743673; https://clinicaltrials.gov/study/NCT05743673.</p>","PeriodicalId":73557,"journal":{"name":"JMIR perioperative medicine","volume":" ","pages":"e65805"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11888076/pdf/","citationCount":"0","resultStr":"{\"title\":\"Implementation of Brief Submaximal Cardiopulmonary Testing in a High-Volume Presurgical Evaluation Clinic: Feasibility Cohort Study.\",\"authors\":\"Zyad James Carr, Daniel Agarkov, Judy Li, Jean Charchaflieh, Andres Brenes-Bastos, Jonah Freund, Jill Zafar, Robert B Schonberger, Paul Heerdt\",\"doi\":\"10.2196/65805\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Precise functional capacity assessment is a critical component for preoperative risk stratification. Brief submaximal cardiopulmonary exercise testing (smCPET) has shown diagnostic utility in various cardiopulmonary conditions.</p><p><strong>Objective: </strong>This study aims to determine if smCPET could be implemented in a high-volume presurgical evaluation clinic and, when compared to structured functional capacity surveys, if smCPET could better discriminate low functional capacity (≤4.6 metabolic equivalents [METs]).</p><p><strong>Methods: </strong>After institutional approval, 43 participants presenting for noncardiac surgery who met the following inclusion criteria were enrolled: aged 60 years and older, a Revised Cardiac Risk Index of ≤2, and self-reported METs of ≥4.6 (self-endorsed ability to climb 2 flights of stairs). Subjective METs assessments, Duke Activity Status Index (DASI) surveys, and a 6-minute smCPET trial were conducted. The primary end points were (1) operational efficiency, based on the time of the experimental session being ≤20 minutes; (2) modified Borg survey of perceived exertion, with a score of ≤7 indicating no more than moderate exertion; (3) high participant satisfaction with smCPET task execution, represented as a score of ≥8 (out of 10); and (4) high participant satisfaction with smCPET scheduling, represented as a score of ≥8 (out of 10). Student's t test was used to determine the significance of the secondary end points. Correlation between comparable structured surveys and smCPET measurements was assessed using the Pearson correlation coefficient. A Bland-Altman analysis was used to assess agreement between the methods.</p><p><strong>Results: </strong>The mean session time was 16.9 (SD 6.8) minutes. The mean posttest modified Borg survey score was 5.35 (SD 1.8). The median patient satisfaction (on a scale of 1=worst to 10=best) was 10 (IQR 10-10) for scheduling and 10 (IQR 9-10) for task execution. Subjective METs were higher when compared to smCPET equivalents (extrapolated peak METs; mean 7.6, SD 2.0 vs mean 6.7, SD 1.8; t<sub>42</sub>=2.1; P<.001). DASI-estimated peak METs were higher when compared to smCPET peak METs (mean 8.8, SD 1.2 vs mean 6.7, SD 1.8; t<sub>42</sub>=7.2; P<.001). DASI-estimated peak oxygen uptake was higher than smCPET peak oxygen uptake (mean 30.9, SD 4.3 mL kg<sup>-1</sup> min<sup>-1</sup> vs mean 23.6, SD 6.5 mL kg<sup>-1</sup> min<sup>-1</sup>; t<sub>42</sub>=7.2; P<.001).</p><p><strong>Conclusions: </strong>Implementation of smCPET in a presurgical evaluation clinic is both patient centered and clinically feasible. Brief smCPET measures, supportive of published reports regarding low sensitivity of provider-driven or structured survey measures for low functional capacity, were lower than those from structured surveys. Future studies will analyze the prediction of perioperative complications and cost-effectiveness.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT05743673; https://clinicaltrials.gov/study/NCT05743673.</p>\",\"PeriodicalId\":73557,\"journal\":{\"name\":\"JMIR perioperative medicine\",\"volume\":\" \",\"pages\":\"e65805\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-02-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11888076/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIR perioperative medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/65805\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR perioperative medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/65805","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:精确的功能能力评估是术前风险分层的关键组成部分。短次最大心肺运动试验(smCPET)已显示出诊断各种心肺疾病的实用价值。目的:本研究的目的是确定smCPET是否可以在大容量的术前评估诊所中实施,并且与结构化功能能力调查相比,smCPET是否可以更好地区分低功能能力(8分)和高参与者对smCPET计划的满意度,得分为bbbb8分(10分)。方法:经机构批准,纳入43例符合以下纳入标准的非心脏手术患者:年龄0 ~ 60岁,修正心脏风险指数4.6(自我认可能爬2段楼梯)。主观METs, Duke活动状态指数(DASI)调查和6分钟smCPET试验进行。使用学生t检验来确定次要终点的显著性。使用Pearson相关系数评估可比较的结构化调查和smCPET测量之间的相关性。使用Bland-Altman分析来评估方法之间的一致性。结果:治疗时间16.9 min(±6.8)。测试后改良Borg测量为5.35(±1.8)。患者满意度中位数(IQR)[从1(最差)到10(最好)]在调度方面为10(10,10),在任务表现方面为10(9,10)。与smCPET等效(外推峰值METs)相比,主观METs更高[7.6(±2.0)vs. 6.7(±1.8),df 42, P
Implementation of Brief Submaximal Cardiopulmonary Testing in a High-Volume Presurgical Evaluation Clinic: Feasibility Cohort Study.
Background: Precise functional capacity assessment is a critical component for preoperative risk stratification. Brief submaximal cardiopulmonary exercise testing (smCPET) has shown diagnostic utility in various cardiopulmonary conditions.
Objective: This study aims to determine if smCPET could be implemented in a high-volume presurgical evaluation clinic and, when compared to structured functional capacity surveys, if smCPET could better discriminate low functional capacity (≤4.6 metabolic equivalents [METs]).
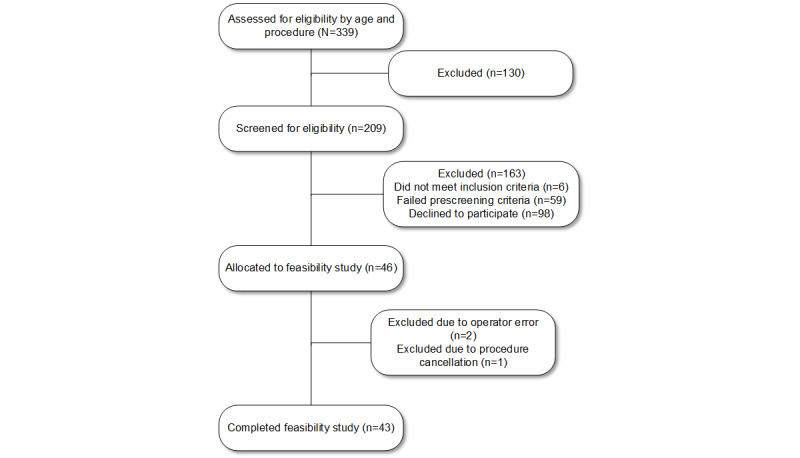
Methods: After institutional approval, 43 participants presenting for noncardiac surgery who met the following inclusion criteria were enrolled: aged 60 years and older, a Revised Cardiac Risk Index of ≤2, and self-reported METs of ≥4.6 (self-endorsed ability to climb 2 flights of stairs). Subjective METs assessments, Duke Activity Status Index (DASI) surveys, and a 6-minute smCPET trial were conducted. The primary end points were (1) operational efficiency, based on the time of the experimental session being ≤20 minutes; (2) modified Borg survey of perceived exertion, with a score of ≤7 indicating no more than moderate exertion; (3) high participant satisfaction with smCPET task execution, represented as a score of ≥8 (out of 10); and (4) high participant satisfaction with smCPET scheduling, represented as a score of ≥8 (out of 10). Student's t test was used to determine the significance of the secondary end points. Correlation between comparable structured surveys and smCPET measurements was assessed using the Pearson correlation coefficient. A Bland-Altman analysis was used to assess agreement between the methods.
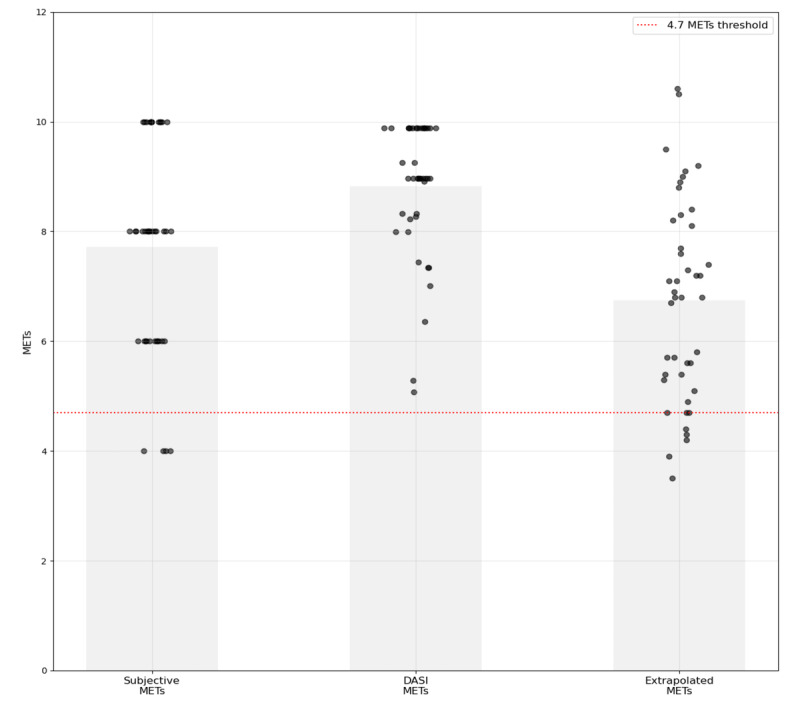
Results: The mean session time was 16.9 (SD 6.8) minutes. The mean posttest modified Borg survey score was 5.35 (SD 1.8). The median patient satisfaction (on a scale of 1=worst to 10=best) was 10 (IQR 10-10) for scheduling and 10 (IQR 9-10) for task execution. Subjective METs were higher when compared to smCPET equivalents (extrapolated peak METs; mean 7.6, SD 2.0 vs mean 6.7, SD 1.8; t42=2.1; P<.001). DASI-estimated peak METs were higher when compared to smCPET peak METs (mean 8.8, SD 1.2 vs mean 6.7, SD 1.8; t42=7.2; P<.001). DASI-estimated peak oxygen uptake was higher than smCPET peak oxygen uptake (mean 30.9, SD 4.3 mL kg-1 min-1 vs mean 23.6, SD 6.5 mL kg-1 min-1; t42=7.2; P<.001).
Conclusions: Implementation of smCPET in a presurgical evaluation clinic is both patient centered and clinically feasible. Brief smCPET measures, supportive of published reports regarding low sensitivity of provider-driven or structured survey measures for low functional capacity, were lower than those from structured surveys. Future studies will analyze the prediction of perioperative complications and cost-effectiveness.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


