Michaela R Cunningham, Christopher L Cramer, Ruyun Jin, Florence E Turrentine, Victor M Zaydfudim
{"title":"预测胃肠手术后老年患者的独立性丧失。","authors":"Michaela R Cunningham, Christopher L Cramer, Ruyun Jin, Florence E Turrentine, Victor M Zaydfudim","doi":"10.1186/s13037-024-00424-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>While existing risk calculators focus on mortality and complications, elderly patients are concerned with how operations will affect their quality of life, especially their independence. We sought to develop a novel clinically relevant and easy-to-use score to predict elderly patients' loss of independence after gastrointestinal surgery.</p><p><strong>Methods: </strong>This retrospective cohort study included patients age ≥ 65 years enrolled in the American College of Surgeons National Surgical Quality Improvement Program database and Geriatric Pilot Project who underwent pancreatic, colorectal, or hepatic surgery (January 1, 2014- December 31, 2018). Primary outcome was loss of independence - discharge to facility other than home and decline in functional status. Patients from 2014 to 2017 comprised the training data set. A logistic regression (LR) model was generated using variables with p < 0.2 from the univariable analysis. The six factors most predictive of the outcome composed the short LR model and scoring system. The scoring system was validated with data from 2018.</p><p><strong>Results: </strong>Of 6,510 operations, 841 patients (13%) lost independence. Training and validation datasets had 5,232 (80%) and 1,278 (20%) patients, respectively. The six most impactful factors in predicting loss of independence were age, preoperative mobility aid use, American Society of Anesthesiologists classification, preoperative albumin, non-elective surgery, and race (all OR > 1.83; p < 0.001). The odds ratio of each of these factors were used to create a sixteen-point scoring system. The scoring system demonstrated satisfactory discrimination and calibration across the training and validation datasets, with Receiver Operating Characteristic Area Under the Curve 0.78 in both and Hosmer-Lemeshow statistic of 0.16 and 0.34, respectively.</p><p><strong>Conclusions: </strong>This novel scoring system predicts loss of independence for geriatric patients after gastrointestinal operations. Using readily available variables, this tool can be applied in the urgent setting and can contribute to elderly patients and their family discussions related to loss of independence prior to high-risk gastrointestinal operations. The applicability of this scoring tool to additional surgical sub-specialties and external validation should be explored in future studies.</p>","PeriodicalId":46782,"journal":{"name":"Patient Safety in Surgery","volume":"19 1","pages":"1"},"PeriodicalIF":2.1000,"publicationDate":"2025-01-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11715953/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predicting loss of independence among geriatric patients following gastrointestinal surgery.\",\"authors\":\"Michaela R Cunningham, Christopher L Cramer, Ruyun Jin, Florence E Turrentine, Victor M Zaydfudim\",\"doi\":\"10.1186/s13037-024-00424-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>While existing risk calculators focus on mortality and complications, elderly patients are concerned with how operations will affect their quality of life, especially their independence. We sought to develop a novel clinically relevant and easy-to-use score to predict elderly patients' loss of independence after gastrointestinal surgery.</p><p><strong>Methods: </strong>This retrospective cohort study included patients age ≥ 65 years enrolled in the American College of Surgeons National Surgical Quality Improvement Program database and Geriatric Pilot Project who underwent pancreatic, colorectal, or hepatic surgery (January 1, 2014- December 31, 2018). Primary outcome was loss of independence - discharge to facility other than home and decline in functional status. Patients from 2014 to 2017 comprised the training data set. A logistic regression (LR) model was generated using variables with p < 0.2 from the univariable analysis. The six factors most predictive of the outcome composed the short LR model and scoring system. The scoring system was validated with data from 2018.</p><p><strong>Results: </strong>Of 6,510 operations, 841 patients (13%) lost independence. Training and validation datasets had 5,232 (80%) and 1,278 (20%) patients, respectively. The six most impactful factors in predicting loss of independence were age, preoperative mobility aid use, American Society of Anesthesiologists classification, preoperative albumin, non-elective surgery, and race (all OR > 1.83; p < 0.001). The odds ratio of each of these factors were used to create a sixteen-point scoring system. The scoring system demonstrated satisfactory discrimination and calibration across the training and validation datasets, with Receiver Operating Characteristic Area Under the Curve 0.78 in both and Hosmer-Lemeshow statistic of 0.16 and 0.34, respectively.</p><p><strong>Conclusions: </strong>This novel scoring system predicts loss of independence for geriatric patients after gastrointestinal operations. Using readily available variables, this tool can be applied in the urgent setting and can contribute to elderly patients and their family discussions related to loss of independence prior to high-risk gastrointestinal operations. The applicability of this scoring tool to additional surgical sub-specialties and external validation should be explored in future studies.</p>\",\"PeriodicalId\":46782,\"journal\":{\"name\":\"Patient Safety in Surgery\",\"volume\":\"19 1\",\"pages\":\"1\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-01-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11715953/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Patient Safety in Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13037-024-00424-w\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Patient Safety in Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13037-024-00424-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
Predicting loss of independence among geriatric patients following gastrointestinal surgery.
Background: While existing risk calculators focus on mortality and complications, elderly patients are concerned with how operations will affect their quality of life, especially their independence. We sought to develop a novel clinically relevant and easy-to-use score to predict elderly patients' loss of independence after gastrointestinal surgery.
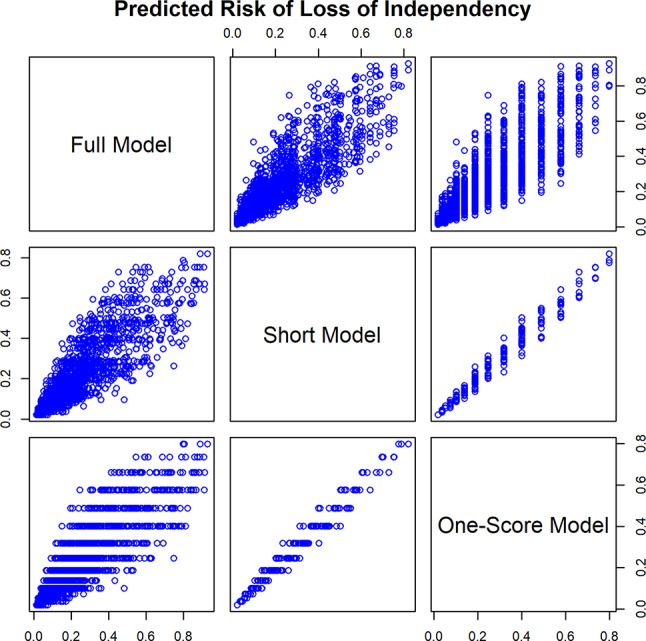
Methods: This retrospective cohort study included patients age ≥ 65 years enrolled in the American College of Surgeons National Surgical Quality Improvement Program database and Geriatric Pilot Project who underwent pancreatic, colorectal, or hepatic surgery (January 1, 2014- December 31, 2018). Primary outcome was loss of independence - discharge to facility other than home and decline in functional status. Patients from 2014 to 2017 comprised the training data set. A logistic regression (LR) model was generated using variables with p < 0.2 from the univariable analysis. The six factors most predictive of the outcome composed the short LR model and scoring system. The scoring system was validated with data from 2018.
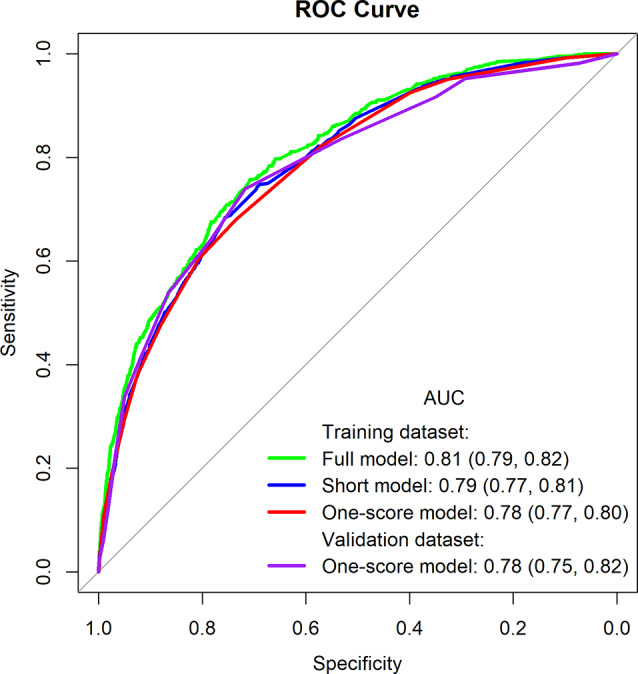
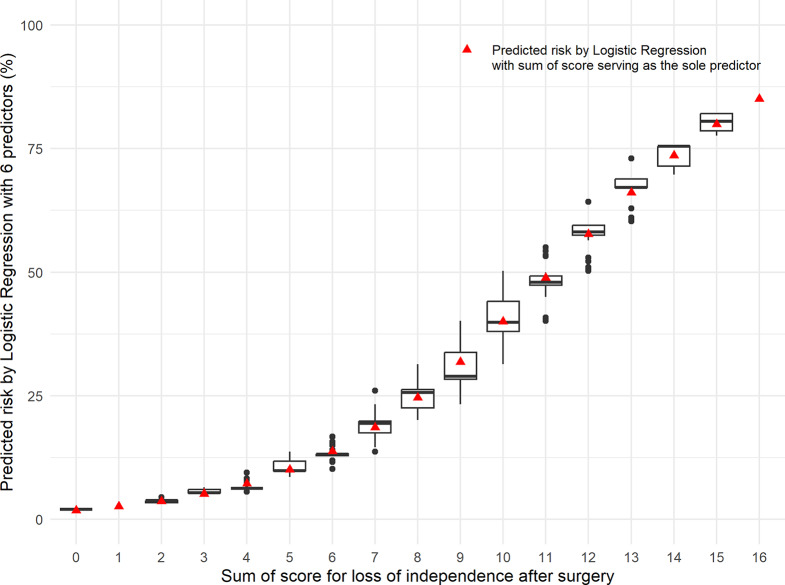
Results: Of 6,510 operations, 841 patients (13%) lost independence. Training and validation datasets had 5,232 (80%) and 1,278 (20%) patients, respectively. The six most impactful factors in predicting loss of independence were age, preoperative mobility aid use, American Society of Anesthesiologists classification, preoperative albumin, non-elective surgery, and race (all OR > 1.83; p < 0.001). The odds ratio of each of these factors were used to create a sixteen-point scoring system. The scoring system demonstrated satisfactory discrimination and calibration across the training and validation datasets, with Receiver Operating Characteristic Area Under the Curve 0.78 in both and Hosmer-Lemeshow statistic of 0.16 and 0.34, respectively.
Conclusions: This novel scoring system predicts loss of independence for geriatric patients after gastrointestinal operations. Using readily available variables, this tool can be applied in the urgent setting and can contribute to elderly patients and their family discussions related to loss of independence prior to high-risk gastrointestinal operations. The applicability of this scoring tool to additional surgical sub-specialties and external validation should be explored in future studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


