{"title":"基于方案的11.7%高渗盐水输注与20%甘露醇输注在颅内压升高患者中的疗效和肾脏安全性:一项随机临床试验的研究方案。","authors":"Sunggyul Lim, Yongjin Yi","doi":"10.5049/EBP.2024.22.2.33","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Elevated intracranial pressure (ICP) is a potentially life-threatening condition requiring prompt intervention. While both mannitol and hypertonic saline (HTS) are commonly used hyperosmotic agents for treating elevated ICP, there is insufficient evidence comparing their renal safety profiles and overall effectiveness. This study protocol outlines a pragmatic randomized trial to compare protocol-based 11.7% HTS with 20% mannitol in patients with elevated ICP, focusing particularly on renal outcomes and treatment efficacy.</p><p><strong>Methods: </strong>This single-center, pragmatic randomized trial will enroll 116 intensive care unit patients with elevated ICP. Participants will be randomly assigned to receive either 11.7% HTS or 20% mannitol following a schedule-based randomization approach, with HTS administration during odd-numbered months and mannitol during even-numbered months. The study will regularly monitor serum electrolytes, osmolarity, and renal function, with brain CT evaluations conducted on days 3 and 7. Comprehensive clinical assessments, including neurological evaluations and laboratory tests, will be performed at specified intervals throughout the study period.</p><p><strong>Measured outcomes: </strong>Primary outcomes include the incidence of acute kidney injury within 7 days according to KDIGO guidelines, requirement for mechanical ventilation, development of pulmonary edema, and significant fluid retention. Secondary outcomes encompass ICU and hospital length of stay, 30- and 90-day mortality rates, and neurological outcomes assessed by Glasgow Coma Scale scores at days 7 and 30. The study hypothesizes that protocol-based HTS administration will demonstrate a lower incidence of acute kidney injury and related complications while maintaining comparable efficacy in managing elevated ICP.</p><p><strong>Conclusion: </strong>This study aims to provide definitive evidence regarding the relative efficacy and safety profiles of HTS compared to mannitol in managing elevated ICP. The findings will help establish clearer clinical guidelines for selecting appropriate hyperosmotic agents, potentially improving patient care outcomes and reducing treatment-related complications. This research will address a significant gap in current clinical knowledge and practice by focusing on treatment efficacy and renal safety considerations in patients with elevated ICP.</p>","PeriodicalId":35352,"journal":{"name":"Electrolyte and Blood Pressure","volume":"22 2","pages":"33-39"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11704315/pdf/","citationCount":"0","resultStr":"{\"title\":\"Efficacy and Renal Safety of Protocol-based 11.7% Hypertonic Saline Infusion Compared with 20% Mannitol in Patients with Elevated Intracranial Pressure: A Study Protocol for a Randomized Clinical Trial.\",\"authors\":\"Sunggyul Lim, Yongjin Yi\",\"doi\":\"10.5049/EBP.2024.22.2.33\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Elevated intracranial pressure (ICP) is a potentially life-threatening condition requiring prompt intervention. While both mannitol and hypertonic saline (HTS) are commonly used hyperosmotic agents for treating elevated ICP, there is insufficient evidence comparing their renal safety profiles and overall effectiveness. This study protocol outlines a pragmatic randomized trial to compare protocol-based 11.7% HTS with 20% mannitol in patients with elevated ICP, focusing particularly on renal outcomes and treatment efficacy.</p><p><strong>Methods: </strong>This single-center, pragmatic randomized trial will enroll 116 intensive care unit patients with elevated ICP. Participants will be randomly assigned to receive either 11.7% HTS or 20% mannitol following a schedule-based randomization approach, with HTS administration during odd-numbered months and mannitol during even-numbered months. The study will regularly monitor serum electrolytes, osmolarity, and renal function, with brain CT evaluations conducted on days 3 and 7. Comprehensive clinical assessments, including neurological evaluations and laboratory tests, will be performed at specified intervals throughout the study period.</p><p><strong>Measured outcomes: </strong>Primary outcomes include the incidence of acute kidney injury within 7 days according to KDIGO guidelines, requirement for mechanical ventilation, development of pulmonary edema, and significant fluid retention. Secondary outcomes encompass ICU and hospital length of stay, 30- and 90-day mortality rates, and neurological outcomes assessed by Glasgow Coma Scale scores at days 7 and 30. The study hypothesizes that protocol-based HTS administration will demonstrate a lower incidence of acute kidney injury and related complications while maintaining comparable efficacy in managing elevated ICP.</p><p><strong>Conclusion: </strong>This study aims to provide definitive evidence regarding the relative efficacy and safety profiles of HTS compared to mannitol in managing elevated ICP. The findings will help establish clearer clinical guidelines for selecting appropriate hyperosmotic agents, potentially improving patient care outcomes and reducing treatment-related complications. This research will address a significant gap in current clinical knowledge and practice by focusing on treatment efficacy and renal safety considerations in patients with elevated ICP.</p>\",\"PeriodicalId\":35352,\"journal\":{\"name\":\"Electrolyte and Blood Pressure\",\"volume\":\"22 2\",\"pages\":\"33-39\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11704315/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Electrolyte and Blood Pressure\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5049/EBP.2024.22.2.33\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Electrolyte and Blood Pressure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5049/EBP.2024.22.2.33","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Efficacy and Renal Safety of Protocol-based 11.7% Hypertonic Saline Infusion Compared with 20% Mannitol in Patients with Elevated Intracranial Pressure: A Study Protocol for a Randomized Clinical Trial.
Background: Elevated intracranial pressure (ICP) is a potentially life-threatening condition requiring prompt intervention. While both mannitol and hypertonic saline (HTS) are commonly used hyperosmotic agents for treating elevated ICP, there is insufficient evidence comparing their renal safety profiles and overall effectiveness. This study protocol outlines a pragmatic randomized trial to compare protocol-based 11.7% HTS with 20% mannitol in patients with elevated ICP, focusing particularly on renal outcomes and treatment efficacy.
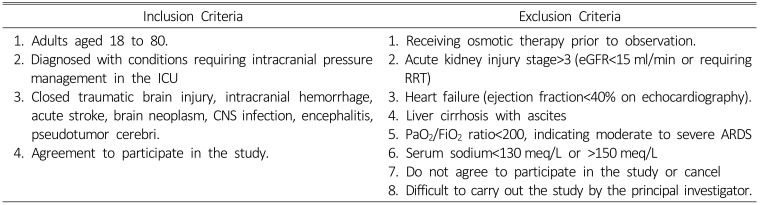
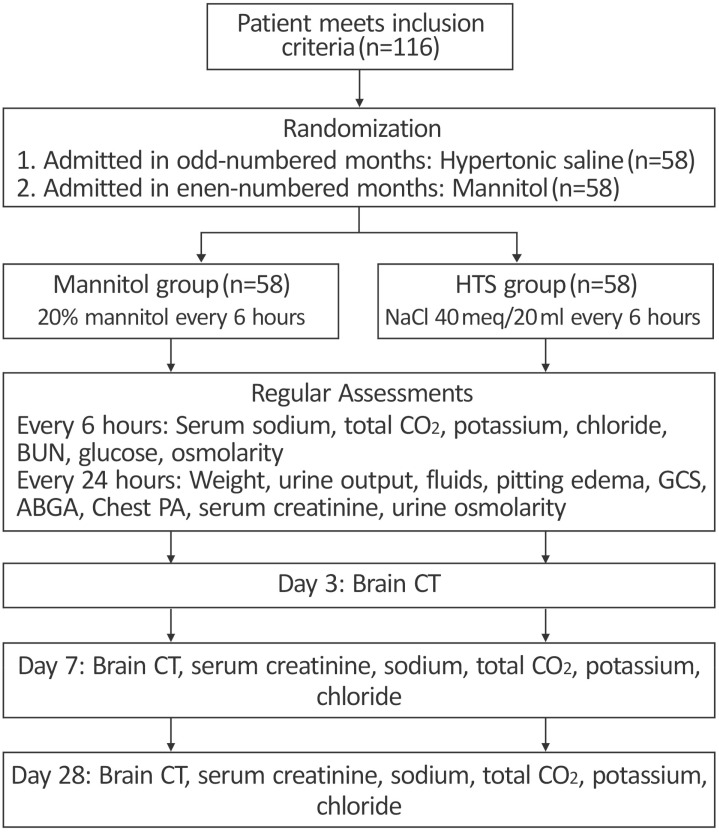
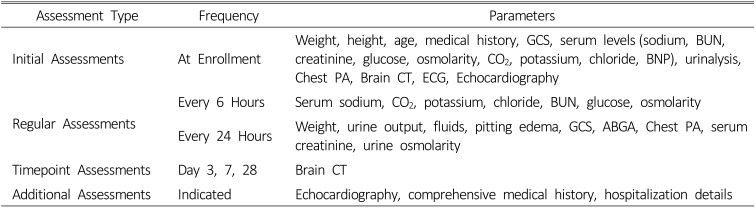
Methods: This single-center, pragmatic randomized trial will enroll 116 intensive care unit patients with elevated ICP. Participants will be randomly assigned to receive either 11.7% HTS or 20% mannitol following a schedule-based randomization approach, with HTS administration during odd-numbered months and mannitol during even-numbered months. The study will regularly monitor serum electrolytes, osmolarity, and renal function, with brain CT evaluations conducted on days 3 and 7. Comprehensive clinical assessments, including neurological evaluations and laboratory tests, will be performed at specified intervals throughout the study period.
Measured outcomes: Primary outcomes include the incidence of acute kidney injury within 7 days according to KDIGO guidelines, requirement for mechanical ventilation, development of pulmonary edema, and significant fluid retention. Secondary outcomes encompass ICU and hospital length of stay, 30- and 90-day mortality rates, and neurological outcomes assessed by Glasgow Coma Scale scores at days 7 and 30. The study hypothesizes that protocol-based HTS administration will demonstrate a lower incidence of acute kidney injury and related complications while maintaining comparable efficacy in managing elevated ICP.
Conclusion: This study aims to provide definitive evidence regarding the relative efficacy and safety profiles of HTS compared to mannitol in managing elevated ICP. The findings will help establish clearer clinical guidelines for selecting appropriate hyperosmotic agents, potentially improving patient care outcomes and reducing treatment-related complications. This research will address a significant gap in current clinical knowledge and practice by focusing on treatment efficacy and renal safety considerations in patients with elevated ICP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


