Derrick Lopez, Juan Lu, Frank M Sanfilippo, Judith M Katzenellenbogen, Tom Briffa, Lee Nedkoff
{"title":"利用行政数据识别和计算冠心病住院治疗次数的比较算法。","authors":"Derrick Lopez, Juan Lu, Frank M Sanfilippo, Judith M Katzenellenbogen, Tom Briffa, Lee Nedkoff","doi":"10.2147/CLEP.S497760","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Measures of disease burden using hospital administrative data are susceptible to over-inflation if the patient is transferred during their episode of care. We aimed to identify and compare measures of coronary heart disease (CHD) and myocardial infarction (MI) episodes using six algorithms that account for transfers.</p><p><strong>Patient and methods: </strong>We used person-linked hospitalisations for CHD and MI for 2000-2016 in Western Australia based on the interval between discharge and subsequent admission (date, datetime algorithms), pathway (admission source, discharge destination) and any combination to generate machine learning models (random forest [RF], gradient boosting machine [GBM]). The date and datetime algorithms used deidentified patient identifiers to identify records belonging to the same individual. We calculated counts, age-standardised rates (ASR) and age-adjusted trends for CHD and MI for each algorithm.</p><p><strong>Results: </strong>Counts of CHD increased from 11,733 in 2000 to 13,274 in 2016, while MI increased from 2605 to 4480 using the date algorithm. Correspondingly ASR for CHD decreased from 2086.2 to 1463.1 while MI increased from 468.2 to 498.1 per 100,000 person-years. ASR for CHD and MI for datetime algorithm were consistently 1-2% higher than the date algorithm. Differences in ASR of CHD and MI counts increased over time with the admission source, RF and GBM algorithms relative to the date algorithm. Age-adjusted trends in CHD and MI episode rates using RF and GBM differed significantly from all other algorithms. Only 86.7% and 87.6% of MI episodes identified by the date algorithm were identified by the admission source and discharge destination algorithms, respectively.</p><p><strong>Conclusion: </strong>The date and datetime algorithms produced the most valid measures of CHD and MI episodes. Findings underscore the importance of identifying admission and discharge dates/times belonging to the same individual in enumerating these episodes.</p>","PeriodicalId":10362,"journal":{"name":"Clinical Epidemiology","volume":"16 ","pages":"921-928"},"PeriodicalIF":3.2000,"publicationDate":"2024-12-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11687321/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparative Algorithms for Identifying and Counting Hospitalisation Episodes of Care for Coronary Heart Disease Using Administrative Data.\",\"authors\":\"Derrick Lopez, Juan Lu, Frank M Sanfilippo, Judith M Katzenellenbogen, Tom Briffa, Lee Nedkoff\",\"doi\":\"10.2147/CLEP.S497760\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Measures of disease burden using hospital administrative data are susceptible to over-inflation if the patient is transferred during their episode of care. We aimed to identify and compare measures of coronary heart disease (CHD) and myocardial infarction (MI) episodes using six algorithms that account for transfers.</p><p><strong>Patient and methods: </strong>We used person-linked hospitalisations for CHD and MI for 2000-2016 in Western Australia based on the interval between discharge and subsequent admission (date, datetime algorithms), pathway (admission source, discharge destination) and any combination to generate machine learning models (random forest [RF], gradient boosting machine [GBM]). The date and datetime algorithms used deidentified patient identifiers to identify records belonging to the same individual. We calculated counts, age-standardised rates (ASR) and age-adjusted trends for CHD and MI for each algorithm.</p><p><strong>Results: </strong>Counts of CHD increased from 11,733 in 2000 to 13,274 in 2016, while MI increased from 2605 to 4480 using the date algorithm. Correspondingly ASR for CHD decreased from 2086.2 to 1463.1 while MI increased from 468.2 to 498.1 per 100,000 person-years. ASR for CHD and MI for datetime algorithm were consistently 1-2% higher than the date algorithm. Differences in ASR of CHD and MI counts increased over time with the admission source, RF and GBM algorithms relative to the date algorithm. Age-adjusted trends in CHD and MI episode rates using RF and GBM differed significantly from all other algorithms. Only 86.7% and 87.6% of MI episodes identified by the date algorithm were identified by the admission source and discharge destination algorithms, respectively.</p><p><strong>Conclusion: </strong>The date and datetime algorithms produced the most valid measures of CHD and MI episodes. Findings underscore the importance of identifying admission and discharge dates/times belonging to the same individual in enumerating these episodes.</p>\",\"PeriodicalId\":10362,\"journal\":{\"name\":\"Clinical Epidemiology\",\"volume\":\"16 \",\"pages\":\"921-928\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2024-12-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11687321/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Epidemiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/CLEP.S497760\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CLEP.S497760","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Comparative Algorithms for Identifying and Counting Hospitalisation Episodes of Care for Coronary Heart Disease Using Administrative Data.
Purpose: Measures of disease burden using hospital administrative data are susceptible to over-inflation if the patient is transferred during their episode of care. We aimed to identify and compare measures of coronary heart disease (CHD) and myocardial infarction (MI) episodes using six algorithms that account for transfers.
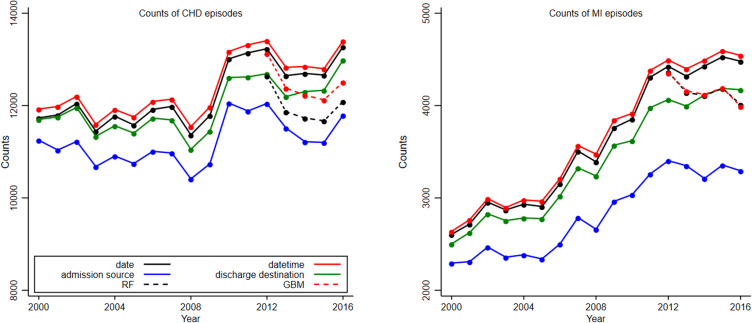
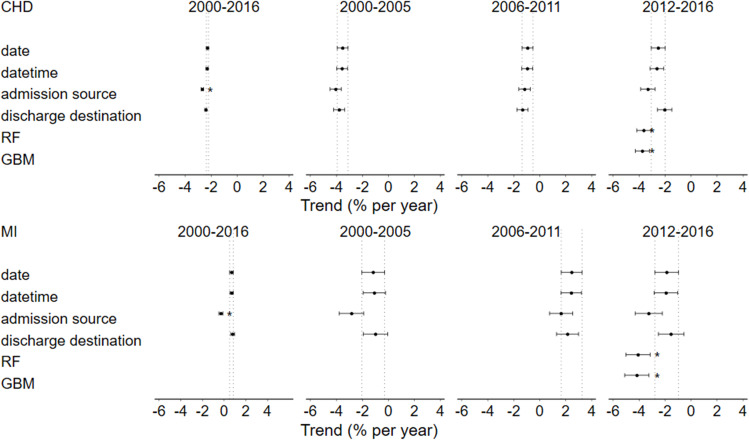
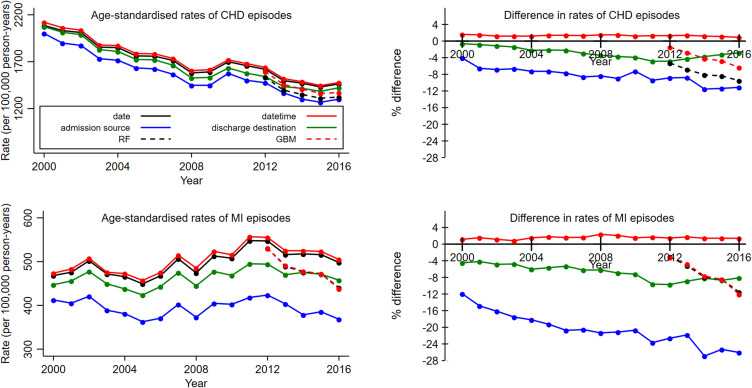
Patient and methods: We used person-linked hospitalisations for CHD and MI for 2000-2016 in Western Australia based on the interval between discharge and subsequent admission (date, datetime algorithms), pathway (admission source, discharge destination) and any combination to generate machine learning models (random forest [RF], gradient boosting machine [GBM]). The date and datetime algorithms used deidentified patient identifiers to identify records belonging to the same individual. We calculated counts, age-standardised rates (ASR) and age-adjusted trends for CHD and MI for each algorithm.
Results: Counts of CHD increased from 11,733 in 2000 to 13,274 in 2016, while MI increased from 2605 to 4480 using the date algorithm. Correspondingly ASR for CHD decreased from 2086.2 to 1463.1 while MI increased from 468.2 to 498.1 per 100,000 person-years. ASR for CHD and MI for datetime algorithm were consistently 1-2% higher than the date algorithm. Differences in ASR of CHD and MI counts increased over time with the admission source, RF and GBM algorithms relative to the date algorithm. Age-adjusted trends in CHD and MI episode rates using RF and GBM differed significantly from all other algorithms. Only 86.7% and 87.6% of MI episodes identified by the date algorithm were identified by the admission source and discharge destination algorithms, respectively.
Conclusion: The date and datetime algorithms produced the most valid measures of CHD and MI episodes. Findings underscore the importance of identifying admission and discharge dates/times belonging to the same individual in enumerating these episodes.
期刊介绍:
Clinical Epidemiology is an international, peer reviewed, open access journal. Clinical Epidemiology focuses on the application of epidemiological principles and questions relating to patients and clinical care in terms of prevention, diagnosis, prognosis, and treatment.
Clinical Epidemiology welcomes papers covering these topics in form of original research and systematic reviews.
Clinical Epidemiology has a special interest in international electronic medical patient records and other routine health care data, especially as applied to safety of medical interventions, clinical utility of diagnostic procedures, understanding short- and long-term clinical course of diseases, clinical epidemiological and biostatistical methods, and systematic reviews.
When considering submission of a paper utilizing publicly-available data, authors should ensure that such studies add significantly to the body of knowledge and that they use appropriate validated methods for identifying health outcomes.
The journal has launched special series describing existing data sources for clinical epidemiology, international health care systems and validation studies of algorithms based on databases and registries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


