Francesco Perna, Francesco Flore, Alessandro Telesca, Eleonora Ruscio, Roberto Scacciavillani, Gianluigi Bencardino, Maria Lucia Narducci, Gaetano Pinnacchio, Gemma Pelargonio
{"title":"超声引导下腋窝静脉穿刺与地标引导入路在心脏植入式电子装置置入中的比较。","authors":"Francesco Perna, Francesco Flore, Alessandro Telesca, Eleonora Ruscio, Roberto Scacciavillani, Gianluigi Bencardino, Maria Lucia Narducci, Gaetano Pinnacchio, Gemma Pelargonio","doi":"10.1111/pace.15107","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Ultrasound (US)-guided axillary vein puncture is a safe and effective approach for cardiac implantable electronic device (CIED) implantation, and it is highly recommended by the current consensus document. However, only reports on small populations are available in the current literature regarding the comparison of this technique with other traditional approaches (subclavian vein blind puncture and cephalic vein surgical cutdown).</p><p><strong>Purpose: </strong>We aimed to assess the effectiveness and safety of US- guided axillary vein puncture using a microintroducer kit for CIED implantation as compared to the aforementioned traditional approaches.</p><p><strong>Methods: </strong>All consecutive patients with an indication to CIED implantation were prospectively enrolled in our observational study from March 2021 to July 2023. Patients were divided into three groups based on venous access route, according to the operator's preference: cephalic vein surgical cutdown (G1), US-guided axillary vein puncture (G2), and subclavian vein blind puncture (G3). Clinical and procedural characteristics, success and complication rates were considered for analysis.</p><p><strong>Results: </strong>A total of 1000 patients (65.2% male, mean age 75.5 ± 10.8 years) were enrolled. Cephalic vein surgical cutdown was chosen in 172 (G1, 17.2%), US-guided axillary access in 433 patients (G2, 43.3%), and subclavian vein in 395 (G3, 39.5%). Success rate was 77.6% in G1, 96.3% in G2, and 97.2% in G3 (G2 vs. G3, p = 0.5; G1 vs. G2, p < 0.0001; G1 vs. G2. vs. G3, p < 0.0001). Compared to subclavian and cephalic groups, in the US-guided axillary group, a successful access was obtained with a reduced mean number of puncture attempts (G2 vs. G3: 1.3 ± 0.9 vs. 1.8 ± 1, p < 0.0001) and needed reduced times to get access (G2 vs. G3: 15 s [10-30 s] vs. 40 [20-65 s]; p < 0.0001, G1 vs. G2: 210 s [180-247 s] vs. 15 s [10-30 s]; p < 0.0001) and to reach the superior vena cava, without differences in total procedural times (72.9 ± 30.4 vs. 75.7 ± 34.8 min, p = 0.24). Bailout fluoroscopy times [1 (0-8) s vs. 20 (10-58) s, p < 0.0001] and usage of vein angiography (11.9% vs. 51.3%, p < 0.0001) were lower in G2 as compared to G3. Complication rate did not differ among the three study groups (early complications: 2.9% in G1, 2.5% in G2, and 2.5% in G3, p = 0.96; late complications: 2.9% in G1, 1.6% in G2, and 0.8% in G3, p = 0.15).</p><p><strong>Conclusions: </strong>US-guided axillary vein puncture for CIED implantation using a microintroducer kit is a safe technique with a very high success rate. Compared to other traditional approaches, it allows to get access with a lower number of puncture attempts and with reduced times, without prolonging the total procedural time. Moreover, x-ray use and need for contrast medium are very rare in US-guided axillary approach. Hence, it should be considered the strategy of choice for most patients undergoing CIED implantation.</p>","PeriodicalId":54653,"journal":{"name":"Pace-Pacing and Clinical Electrophysiology","volume":" ","pages":"9-20"},"PeriodicalIF":1.3000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11708441/pdf/","citationCount":"0","resultStr":"{\"title\":\"Ultrasound-Guided Axillary Vein Puncture Versus Landmark-Guided Approach for Cardiac Implantable Electronic Device Placement.\",\"authors\":\"Francesco Perna, Francesco Flore, Alessandro Telesca, Eleonora Ruscio, Roberto Scacciavillani, Gianluigi Bencardino, Maria Lucia Narducci, Gaetano Pinnacchio, Gemma Pelargonio\",\"doi\":\"10.1111/pace.15107\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Ultrasound (US)-guided axillary vein puncture is a safe and effective approach for cardiac implantable electronic device (CIED) implantation, and it is highly recommended by the current consensus document. However, only reports on small populations are available in the current literature regarding the comparison of this technique with other traditional approaches (subclavian vein blind puncture and cephalic vein surgical cutdown).</p><p><strong>Purpose: </strong>We aimed to assess the effectiveness and safety of US- guided axillary vein puncture using a microintroducer kit for CIED implantation as compared to the aforementioned traditional approaches.</p><p><strong>Methods: </strong>All consecutive patients with an indication to CIED implantation were prospectively enrolled in our observational study from March 2021 to July 2023. Patients were divided into three groups based on venous access route, according to the operator's preference: cephalic vein surgical cutdown (G1), US-guided axillary vein puncture (G2), and subclavian vein blind puncture (G3). Clinical and procedural characteristics, success and complication rates were considered for analysis.</p><p><strong>Results: </strong>A total of 1000 patients (65.2% male, mean age 75.5 ± 10.8 years) were enrolled. Cephalic vein surgical cutdown was chosen in 172 (G1, 17.2%), US-guided axillary access in 433 patients (G2, 43.3%), and subclavian vein in 395 (G3, 39.5%). Success rate was 77.6% in G1, 96.3% in G2, and 97.2% in G3 (G2 vs. G3, p = 0.5; G1 vs. G2, p < 0.0001; G1 vs. G2. vs. G3, p < 0.0001). Compared to subclavian and cephalic groups, in the US-guided axillary group, a successful access was obtained with a reduced mean number of puncture attempts (G2 vs. G3: 1.3 ± 0.9 vs. 1.8 ± 1, p < 0.0001) and needed reduced times to get access (G2 vs. G3: 15 s [10-30 s] vs. 40 [20-65 s]; p < 0.0001, G1 vs. G2: 210 s [180-247 s] vs. 15 s [10-30 s]; p < 0.0001) and to reach the superior vena cava, without differences in total procedural times (72.9 ± 30.4 vs. 75.7 ± 34.8 min, p = 0.24). Bailout fluoroscopy times [1 (0-8) s vs. 20 (10-58) s, p < 0.0001] and usage of vein angiography (11.9% vs. 51.3%, p < 0.0001) were lower in G2 as compared to G3. Complication rate did not differ among the three study groups (early complications: 2.9% in G1, 2.5% in G2, and 2.5% in G3, p = 0.96; late complications: 2.9% in G1, 1.6% in G2, and 0.8% in G3, p = 0.15).</p><p><strong>Conclusions: </strong>US-guided axillary vein puncture for CIED implantation using a microintroducer kit is a safe technique with a very high success rate. Compared to other traditional approaches, it allows to get access with a lower number of puncture attempts and with reduced times, without prolonging the total procedural time. Moreover, x-ray use and need for contrast medium are very rare in US-guided axillary approach. Hence, it should be considered the strategy of choice for most patients undergoing CIED implantation.</p>\",\"PeriodicalId\":54653,\"journal\":{\"name\":\"Pace-Pacing and Clinical Electrophysiology\",\"volume\":\" \",\"pages\":\"9-20\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11708441/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pace-Pacing and Clinical Electrophysiology\",\"FirstCategoryId\":\"5\",\"ListUrlMain\":\"https://doi.org/10.1111/pace.15107\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pace-Pacing and Clinical Electrophysiology","FirstCategoryId":"5","ListUrlMain":"https://doi.org/10.1111/pace.15107","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
导读:超声引导下腋窝静脉穿刺是一种安全有效的心脏植入式电子装置(CIED)植入术,是目前文献一致推荐的方法。然而,在目前的文献中,关于该技术与其他传统方法(锁骨下静脉盲穿刺和头静脉手术切断)的比较,只有少数人群的报道。目的:我们的目的是评估与上述传统方法相比,使用微引入器套件进行US引导腋窝静脉穿刺用于CIED植入的有效性和安全性。方法:从2021年3月至2023年7月,所有有CIED植入指征的连续患者前瞻性纳入我们的观察性研究。根据操作者喜好,将患者根据静脉通路分为头静脉手术切断组(G1)、us引导下腋窝静脉穿刺组(G2)、锁骨下静脉盲穿刺组(G3)。临床和手术特点,成功率和并发症发生率进行分析。结果:共纳入1000例患者,其中男性占65.2%,平均年龄75.5±10.8岁。手术切断头静脉172例(G1, 17.2%), us引导下腋静脉433例(G2, 43.3%),锁骨下静脉395例(G3, 39.5%)。G1、G2、G3的成功率分别为77.6%、96.3%、97.2% (G2 vs. G3, p = 0.5;结论:us引导下腋窝静脉穿刺使用微导入器试剂盒植入CIED是一种安全的技术,成功率很高。与其他传统方法相比,它可以减少穿刺次数和次数,而不会延长总手术时间。此外,x线的使用和造影剂的需要在美国引导下腋窝入路是非常罕见的。因此,对于大多数接受CIED植入术的患者来说,这应该是一种选择策略。
Ultrasound-Guided Axillary Vein Puncture Versus Landmark-Guided Approach for Cardiac Implantable Electronic Device Placement.
Introduction: Ultrasound (US)-guided axillary vein puncture is a safe and effective approach for cardiac implantable electronic device (CIED) implantation, and it is highly recommended by the current consensus document. However, only reports on small populations are available in the current literature regarding the comparison of this technique with other traditional approaches (subclavian vein blind puncture and cephalic vein surgical cutdown).
Purpose: We aimed to assess the effectiveness and safety of US- guided axillary vein puncture using a microintroducer kit for CIED implantation as compared to the aforementioned traditional approaches.
Methods: All consecutive patients with an indication to CIED implantation were prospectively enrolled in our observational study from March 2021 to July 2023. Patients were divided into three groups based on venous access route, according to the operator's preference: cephalic vein surgical cutdown (G1), US-guided axillary vein puncture (G2), and subclavian vein blind puncture (G3). Clinical and procedural characteristics, success and complication rates were considered for analysis.
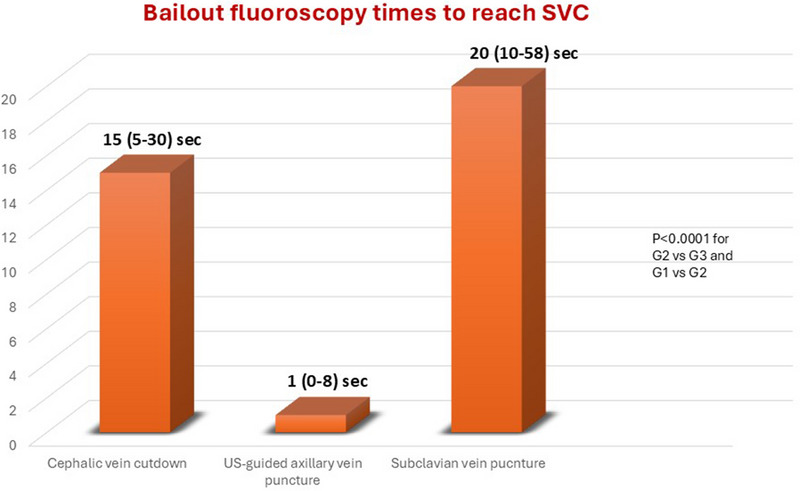
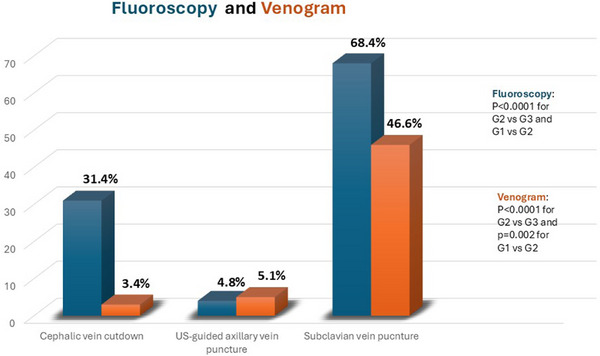
Results: A total of 1000 patients (65.2% male, mean age 75.5 ± 10.8 years) were enrolled. Cephalic vein surgical cutdown was chosen in 172 (G1, 17.2%), US-guided axillary access in 433 patients (G2, 43.3%), and subclavian vein in 395 (G3, 39.5%). Success rate was 77.6% in G1, 96.3% in G2, and 97.2% in G3 (G2 vs. G3, p = 0.5; G1 vs. G2, p < 0.0001; G1 vs. G2. vs. G3, p < 0.0001). Compared to subclavian and cephalic groups, in the US-guided axillary group, a successful access was obtained with a reduced mean number of puncture attempts (G2 vs. G3: 1.3 ± 0.9 vs. 1.8 ± 1, p < 0.0001) and needed reduced times to get access (G2 vs. G3: 15 s [10-30 s] vs. 40 [20-65 s]; p < 0.0001, G1 vs. G2: 210 s [180-247 s] vs. 15 s [10-30 s]; p < 0.0001) and to reach the superior vena cava, without differences in total procedural times (72.9 ± 30.4 vs. 75.7 ± 34.8 min, p = 0.24). Bailout fluoroscopy times [1 (0-8) s vs. 20 (10-58) s, p < 0.0001] and usage of vein angiography (11.9% vs. 51.3%, p < 0.0001) were lower in G2 as compared to G3. Complication rate did not differ among the three study groups (early complications: 2.9% in G1, 2.5% in G2, and 2.5% in G3, p = 0.96; late complications: 2.9% in G1, 1.6% in G2, and 0.8% in G3, p = 0.15).
Conclusions: US-guided axillary vein puncture for CIED implantation using a microintroducer kit is a safe technique with a very high success rate. Compared to other traditional approaches, it allows to get access with a lower number of puncture attempts and with reduced times, without prolonging the total procedural time. Moreover, x-ray use and need for contrast medium are very rare in US-guided axillary approach. Hence, it should be considered the strategy of choice for most patients undergoing CIED implantation.
期刊介绍:
Pacing and Clinical Electrophysiology (PACE) is the foremost peer-reviewed journal in the field of pacing and implantable cardioversion defibrillation, publishing over 50% of all English language articles in its field, featuring original, review, and didactic papers, and case reports related to daily practice. Articles also include editorials, book reviews, Musings on humane topics relevant to medical practice, electrophysiology (EP) rounds, device rounds, and information concerning the quality of devices used in the practice of the specialty.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


