{"title":"早期姑息治疗干预对临终病人医疗资源使用的影响。","authors":"Chia-Chia Lin, Tsing-Fen Ho, Chang-Hung Lin, Nu-Man Tsai, Yu-Hung Kuo, Ju-Huei Chien","doi":"10.1093/intqhc/mzae119","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In Taiwan, as the population ages, palliative care services (PCS) have expanded significantly to include comprehensive benefit plans for critically ill individuals, supported by reimbursements from the National Health Insurance program. However, incorporating palliative care into the medical management of these patients presents several challenges. We aim to evaluate the effects of palliative care interventions on medical resources in end-of-life scenarios, to promote earlier palliative care access and provide high-quality healthcare services for patients.</p><p><strong>Methods: </strong>A total of 2202 patients were included in this study. Primary diagnosis and referral for PCS were assessed using ICD-10 and HNI code. All study subjects were divided into three groups: patients who did not receive PCS (no-PCS), patients who received PCS before their final hospital admission (PCS-before), and patients who received PCS after their final admission (PCS-after). We evaluated (i) the effects of PCS on eight medical resource utilization outcomes within the 30 days preceding death and (ii) the effects of early intervention on two major diseases.</p><p><strong>Results: </strong>Initiating PCS before a patient's last hospital admission was associated with less aggressive medical interventions in the 30 days before death, including reduced length of intensive care unit (ICU) [odds ratio (OR) = 0.25], and rates of endotracheal intubation (OR = 0.12), respiratory ventilator support (OR = 0.20), cardiopulmonary resuscitation (OR = 0.18), and blood transfusion (OR = 0.65). Among patients with cancer and lung diseases, those who received PCS prior to their final hospitalization of over 14 days experienced reduced hospitalization duration (OR = 0.52 and 0.24, respectively). Patients with lung disease also had significantly lower odds of ICU stays (OR = 0.44) and respiratory ventilation (OR = 0.33).</p><p><strong>Conclusion: </strong>The timing of palliative care intervention critically impacts on duration of hospitalization and ICU stay and the need for intubation procedures or cardiopulmonary resuscitation. The findings can help the government and medical providers in developing comprehensive palliative care policies and programs to improve care quality and patient rights.</p>","PeriodicalId":13800,"journal":{"name":"International Journal for Quality in Health Care","volume":" ","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2025-01-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11711585/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of early palliative care intervention on medical resource use among end-of-life patients.\",\"authors\":\"Chia-Chia Lin, Tsing-Fen Ho, Chang-Hung Lin, Nu-Man Tsai, Yu-Hung Kuo, Ju-Huei Chien\",\"doi\":\"10.1093/intqhc/mzae119\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In Taiwan, as the population ages, palliative care services (PCS) have expanded significantly to include comprehensive benefit plans for critically ill individuals, supported by reimbursements from the National Health Insurance program. However, incorporating palliative care into the medical management of these patients presents several challenges. We aim to evaluate the effects of palliative care interventions on medical resources in end-of-life scenarios, to promote earlier palliative care access and provide high-quality healthcare services for patients.</p><p><strong>Methods: </strong>A total of 2202 patients were included in this study. Primary diagnosis and referral for PCS were assessed using ICD-10 and HNI code. All study subjects were divided into three groups: patients who did not receive PCS (no-PCS), patients who received PCS before their final hospital admission (PCS-before), and patients who received PCS after their final admission (PCS-after). We evaluated (i) the effects of PCS on eight medical resource utilization outcomes within the 30 days preceding death and (ii) the effects of early intervention on two major diseases.</p><p><strong>Results: </strong>Initiating PCS before a patient's last hospital admission was associated with less aggressive medical interventions in the 30 days before death, including reduced length of intensive care unit (ICU) [odds ratio (OR) = 0.25], and rates of endotracheal intubation (OR = 0.12), respiratory ventilator support (OR = 0.20), cardiopulmonary resuscitation (OR = 0.18), and blood transfusion (OR = 0.65). Among patients with cancer and lung diseases, those who received PCS prior to their final hospitalization of over 14 days experienced reduced hospitalization duration (OR = 0.52 and 0.24, respectively). Patients with lung disease also had significantly lower odds of ICU stays (OR = 0.44) and respiratory ventilation (OR = 0.33).</p><p><strong>Conclusion: </strong>The timing of palliative care intervention critically impacts on duration of hospitalization and ICU stay and the need for intubation procedures or cardiopulmonary resuscitation. The findings can help the government and medical providers in developing comprehensive palliative care policies and programs to improve care quality and patient rights.</p>\",\"PeriodicalId\":13800,\"journal\":{\"name\":\"International Journal for Quality in Health Care\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-01-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11711585/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal for Quality in Health Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/intqhc/mzae119\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal for Quality in Health Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/intqhc/mzae119","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Effects of early palliative care intervention on medical resource use among end-of-life patients.
Background: In Taiwan, as the population ages, palliative care services (PCS) have expanded significantly to include comprehensive benefit plans for critically ill individuals, supported by reimbursements from the National Health Insurance program. However, incorporating palliative care into the medical management of these patients presents several challenges. We aim to evaluate the effects of palliative care interventions on medical resources in end-of-life scenarios, to promote earlier palliative care access and provide high-quality healthcare services for patients.
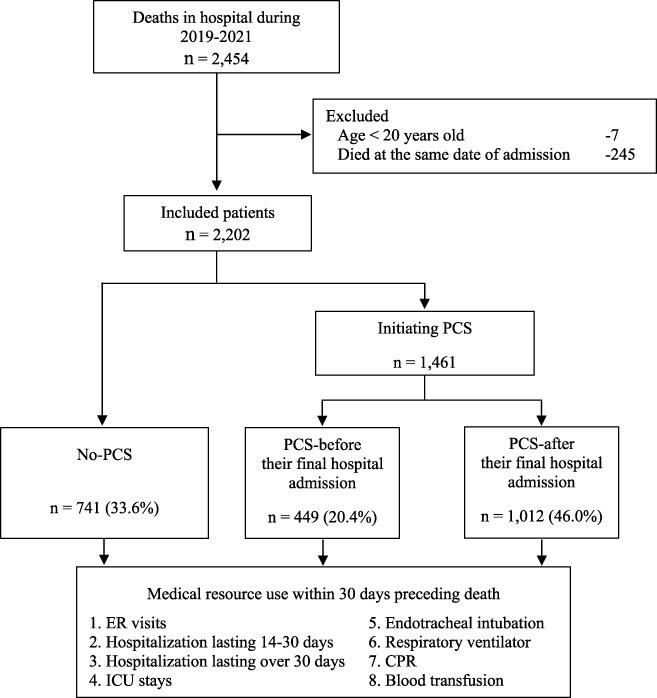
Methods: A total of 2202 patients were included in this study. Primary diagnosis and referral for PCS were assessed using ICD-10 and HNI code. All study subjects were divided into three groups: patients who did not receive PCS (no-PCS), patients who received PCS before their final hospital admission (PCS-before), and patients who received PCS after their final admission (PCS-after). We evaluated (i) the effects of PCS on eight medical resource utilization outcomes within the 30 days preceding death and (ii) the effects of early intervention on two major diseases.
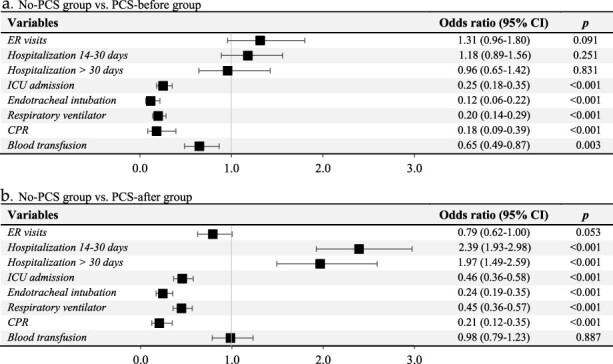
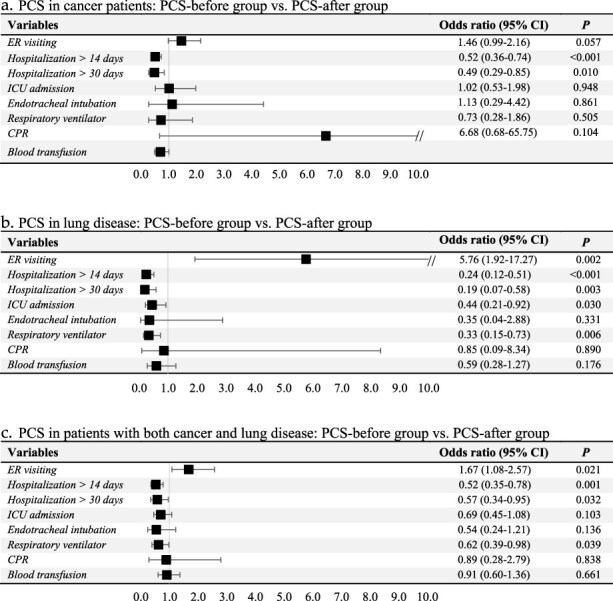
Results: Initiating PCS before a patient's last hospital admission was associated with less aggressive medical interventions in the 30 days before death, including reduced length of intensive care unit (ICU) [odds ratio (OR) = 0.25], and rates of endotracheal intubation (OR = 0.12), respiratory ventilator support (OR = 0.20), cardiopulmonary resuscitation (OR = 0.18), and blood transfusion (OR = 0.65). Among patients with cancer and lung diseases, those who received PCS prior to their final hospitalization of over 14 days experienced reduced hospitalization duration (OR = 0.52 and 0.24, respectively). Patients with lung disease also had significantly lower odds of ICU stays (OR = 0.44) and respiratory ventilation (OR = 0.33).
Conclusion: The timing of palliative care intervention critically impacts on duration of hospitalization and ICU stay and the need for intubation procedures or cardiopulmonary resuscitation. The findings can help the government and medical providers in developing comprehensive palliative care policies and programs to improve care quality and patient rights.
期刊介绍:
The International Journal for Quality in Health Care makes activities and research related to quality and safety in health care available to a worldwide readership. The Journal publishes papers in all disciplines related to the quality and safety of health care, including health services research, health care evaluation, technology assessment, health economics, utilization review, cost containment, and nursing care research, as well as clinical research related to quality of care.
This peer-reviewed journal is truly interdisciplinary and includes contributions from representatives of all health professions such as doctors, nurses, quality assurance professionals, managers, politicians, social workers, and therapists, as well as researchers from health-related backgrounds.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


