Clemens Miller, Anselm Bräuer, Johannes Wieditz, Marcus Nemeth
{"title":"儿科麻醉术中核心体温测量报告的最小时间间隔是多少?二次分析。","authors":"Clemens Miller, Anselm Bräuer, Johannes Wieditz, Marcus Nemeth","doi":"10.1007/s10877-024-01254-y","DOIUrl":null,"url":null,"abstract":"<p><p>Given that perioperative normothermia represents a quality parameter in pediatric anesthesia, numerous studies have been conducted on temperature measurement, albeit with heterogeneous measurement intervals, ranging from 30 s to fifteen minutes. We aimed to determine the minimum time interval for reporting of intraoperative core body temperature across commonly used measurement intervals in children. Data were extracted from the records of 65 children who had participated in another clinical study and analyzed using a quasibinomial mixed linear model. Documented artifacts, like probe dislocations or at the end of anesthesia, were removed. Primary outcome was the respective probability of failing to detect a temperature change of 0.2 °C or more at any one measurement point at 30 s, one minute, two minutes, five minutes, ten minutes, and fifteen minutes, considering an expected probability of less than 5% to be acceptable. Secondary outcomes included the probabilities of failing to detect hypothermia (< 36.0 °C) and hyperthermia (> 38.0 °C). Following the removal of 4,909 exclusions, the remaining 222,366 timestamped measurements (representing just over 60 h of monitoring) were analyzed. The median measurement time was 45 min. The expected probabilities of failing to detect a temperature change of 0.2 °C or more were 0.2% [95%-CI 0.0-0.7], 0.5% [95%-CI 0.0-1.2], 1.5% [95%-CI 0.2-2.6], 4.8% [95%-CI 2.7-6.9], 22.4% [95%-CI 18.3-26.4], and 31.9% [95%-CI 27.3-36.4], respectively. Probabilities for the detection of hyperthermia (n = 9) were lower and omitted for hypothermia due to low prevalence (n = 1). In conclusion, the core body temperature should be reported at intervals of no more than five minutes to ensure the detection of any temperature change in normothermic ranges. Further studies should focus on hypothermic and hyperthermic ranges.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"1101-1108"},"PeriodicalIF":2.2000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12474714/pdf/","citationCount":"0","resultStr":"{\"title\":\"What is the minimum time interval for reporting of intraoperative core body temperature measurements in pediatric anesthesia? A secondary analysis.\",\"authors\":\"Clemens Miller, Anselm Bräuer, Johannes Wieditz, Marcus Nemeth\",\"doi\":\"10.1007/s10877-024-01254-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Given that perioperative normothermia represents a quality parameter in pediatric anesthesia, numerous studies have been conducted on temperature measurement, albeit with heterogeneous measurement intervals, ranging from 30 s to fifteen minutes. We aimed to determine the minimum time interval for reporting of intraoperative core body temperature across commonly used measurement intervals in children. Data were extracted from the records of 65 children who had participated in another clinical study and analyzed using a quasibinomial mixed linear model. Documented artifacts, like probe dislocations or at the end of anesthesia, were removed. Primary outcome was the respective probability of failing to detect a temperature change of 0.2 °C or more at any one measurement point at 30 s, one minute, two minutes, five minutes, ten minutes, and fifteen minutes, considering an expected probability of less than 5% to be acceptable. Secondary outcomes included the probabilities of failing to detect hypothermia (< 36.0 °C) and hyperthermia (> 38.0 °C). Following the removal of 4,909 exclusions, the remaining 222,366 timestamped measurements (representing just over 60 h of monitoring) were analyzed. The median measurement time was 45 min. The expected probabilities of failing to detect a temperature change of 0.2 °C or more were 0.2% [95%-CI 0.0-0.7], 0.5% [95%-CI 0.0-1.2], 1.5% [95%-CI 0.2-2.6], 4.8% [95%-CI 2.7-6.9], 22.4% [95%-CI 18.3-26.4], and 31.9% [95%-CI 27.3-36.4], respectively. Probabilities for the detection of hyperthermia (n = 9) were lower and omitted for hypothermia due to low prevalence (n = 1). In conclusion, the core body temperature should be reported at intervals of no more than five minutes to ensure the detection of any temperature change in normothermic ranges. Further studies should focus on hypothermic and hyperthermic ranges.</p>\",\"PeriodicalId\":15513,\"journal\":{\"name\":\"Journal of Clinical Monitoring and Computing\",\"volume\":\" \",\"pages\":\"1101-1108\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12474714/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Monitoring and Computing\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10877-024-01254-y\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/19 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-024-01254-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/19 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
What is the minimum time interval for reporting of intraoperative core body temperature measurements in pediatric anesthesia? A secondary analysis.
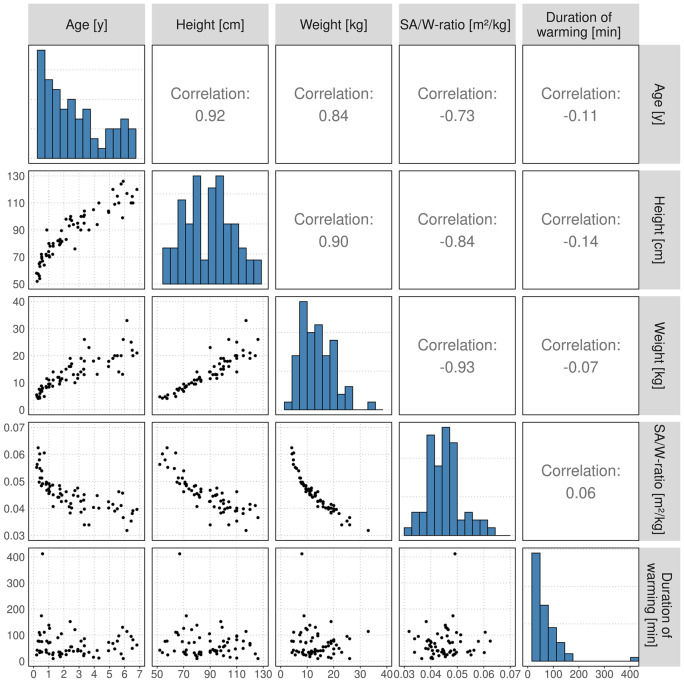
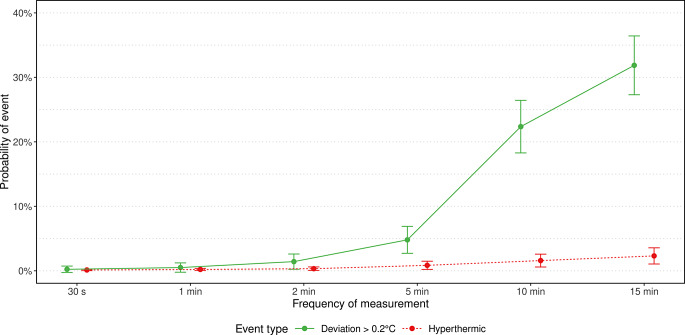
Given that perioperative normothermia represents a quality parameter in pediatric anesthesia, numerous studies have been conducted on temperature measurement, albeit with heterogeneous measurement intervals, ranging from 30 s to fifteen minutes. We aimed to determine the minimum time interval for reporting of intraoperative core body temperature across commonly used measurement intervals in children. Data were extracted from the records of 65 children who had participated in another clinical study and analyzed using a quasibinomial mixed linear model. Documented artifacts, like probe dislocations or at the end of anesthesia, were removed. Primary outcome was the respective probability of failing to detect a temperature change of 0.2 °C or more at any one measurement point at 30 s, one minute, two minutes, five minutes, ten minutes, and fifteen minutes, considering an expected probability of less than 5% to be acceptable. Secondary outcomes included the probabilities of failing to detect hypothermia (< 36.0 °C) and hyperthermia (> 38.0 °C). Following the removal of 4,909 exclusions, the remaining 222,366 timestamped measurements (representing just over 60 h of monitoring) were analyzed. The median measurement time was 45 min. The expected probabilities of failing to detect a temperature change of 0.2 °C or more were 0.2% [95%-CI 0.0-0.7], 0.5% [95%-CI 0.0-1.2], 1.5% [95%-CI 0.2-2.6], 4.8% [95%-CI 2.7-6.9], 22.4% [95%-CI 18.3-26.4], and 31.9% [95%-CI 27.3-36.4], respectively. Probabilities for the detection of hyperthermia (n = 9) were lower and omitted for hypothermia due to low prevalence (n = 1). In conclusion, the core body temperature should be reported at intervals of no more than five minutes to ensure the detection of any temperature change in normothermic ranges. Further studies should focus on hypothermic and hyperthermic ranges.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


