Daniel L Miller, Jacob Hutchins, Michael A Ferguson, Yazid Barhoush, Emily Achter, John P Kuckelman
{"title":"肺叶切除术中肋间神经冷冻消融治疗手术后疼痛:一种安全且经济有效的干预措施","authors":"Daniel L Miller, Jacob Hutchins, Michael A Ferguson, Yazid Barhoush, Emily Achter, John P Kuckelman","doi":"10.1007/s40122-024-00694-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The cost benefit of intercostal nerve cryoablation during surgical lobectomy for postoperative pain management is unknown. The current study compared hospital economics, resource use, and clinical outcomes during the index stay and accompanying short-term follow-up. Patients who underwent lobectomy with standard of care treatment for postsurgical pain management and cryoablation were compared to those with standard of care treatment only. We hypothesized that cryoablation would reduce narcotic use and index hospital and short-term costs.</p><p><strong>Methods: </strong>A retrospective, propensity matched cohort of surgical patients treated between 2016 and 2022 from a US National All-Payer Database were used. Cost and outcome comparisons were made between groups using chi-square and t tests.</p><p><strong>Results: </strong>From a cohort of 23,138 patients, 266 pairs with a mean age of 69 years were included. Matching variables included age, gender, lobe resected, and prior opioid use. Both groups had significant comorbidity history and prior opioid use; 66% (n = 175 both groups) underwent open lobectomy and 53% (n = 142 vs. 143) had the upper lobe resected. Cryoablation intervention was associated with 1.3 days reduced hospital stay (8.8 vs. 10.1 days, p = 0.31) and no difference in perioperative safety. After 90 days, postsurgery cryoablation patients had lower opioid prescription refills (27.3 vs. 36.9 morphine milligram equivalents, p = 0.03). Cryoablation patient costs trended less than non-cryoablation patients during index ($38,753 vs. $43,974, p = 0.10) and lower through 6 months (total costs, $65,703 vs. $74,304, p = 0.10). There was no difference in postsurgery resource use, but a smaller proportion of cryoablation patients had outpatient hospital visits (83.1%, N = 221 vs. 92.9%, n = 247, p < 0.01).</p><p><strong>Conclusion: </strong>Cryoablation during lobectomy is safe and does not add incremental hospital costs. Clinical meaningful reductions in length of stay and postsurgery opioid use were observed with cryoablation intervention. The addition of cryoablation during surgery to reduce postoperative pain appears to be a cost-effective therapy.</p>","PeriodicalId":19908,"journal":{"name":"Pain and Therapy","volume":" ","pages":"317-328"},"PeriodicalIF":3.3000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11751353/pdf/","citationCount":"0","resultStr":"{\"title\":\"Intercostal Nerve Cryoablation During Lobectomy for Postsurgical Pain: A Safe and Cost-Effective Intervention.\",\"authors\":\"Daniel L Miller, Jacob Hutchins, Michael A Ferguson, Yazid Barhoush, Emily Achter, John P Kuckelman\",\"doi\":\"10.1007/s40122-024-00694-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The cost benefit of intercostal nerve cryoablation during surgical lobectomy for postoperative pain management is unknown. The current study compared hospital economics, resource use, and clinical outcomes during the index stay and accompanying short-term follow-up. Patients who underwent lobectomy with standard of care treatment for postsurgical pain management and cryoablation were compared to those with standard of care treatment only. We hypothesized that cryoablation would reduce narcotic use and index hospital and short-term costs.</p><p><strong>Methods: </strong>A retrospective, propensity matched cohort of surgical patients treated between 2016 and 2022 from a US National All-Payer Database were used. Cost and outcome comparisons were made between groups using chi-square and t tests.</p><p><strong>Results: </strong>From a cohort of 23,138 patients, 266 pairs with a mean age of 69 years were included. Matching variables included age, gender, lobe resected, and prior opioid use. Both groups had significant comorbidity history and prior opioid use; 66% (n = 175 both groups) underwent open lobectomy and 53% (n = 142 vs. 143) had the upper lobe resected. Cryoablation intervention was associated with 1.3 days reduced hospital stay (8.8 vs. 10.1 days, p = 0.31) and no difference in perioperative safety. After 90 days, postsurgery cryoablation patients had lower opioid prescription refills (27.3 vs. 36.9 morphine milligram equivalents, p = 0.03). Cryoablation patient costs trended less than non-cryoablation patients during index ($38,753 vs. $43,974, p = 0.10) and lower through 6 months (total costs, $65,703 vs. $74,304, p = 0.10). There was no difference in postsurgery resource use, but a smaller proportion of cryoablation patients had outpatient hospital visits (83.1%, N = 221 vs. 92.9%, n = 247, p < 0.01).</p><p><strong>Conclusion: </strong>Cryoablation during lobectomy is safe and does not add incremental hospital costs. Clinical meaningful reductions in length of stay and postsurgery opioid use were observed with cryoablation intervention. The addition of cryoablation during surgery to reduce postoperative pain appears to be a cost-effective therapy.</p>\",\"PeriodicalId\":19908,\"journal\":{\"name\":\"Pain and Therapy\",\"volume\":\" \",\"pages\":\"317-328\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2025-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11751353/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pain and Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40122-024-00694-3\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pain and Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40122-024-00694-3","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/17 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Intercostal Nerve Cryoablation During Lobectomy for Postsurgical Pain: A Safe and Cost-Effective Intervention.
Introduction: The cost benefit of intercostal nerve cryoablation during surgical lobectomy for postoperative pain management is unknown. The current study compared hospital economics, resource use, and clinical outcomes during the index stay and accompanying short-term follow-up. Patients who underwent lobectomy with standard of care treatment for postsurgical pain management and cryoablation were compared to those with standard of care treatment only. We hypothesized that cryoablation would reduce narcotic use and index hospital and short-term costs.
Methods: A retrospective, propensity matched cohort of surgical patients treated between 2016 and 2022 from a US National All-Payer Database were used. Cost and outcome comparisons were made between groups using chi-square and t tests.
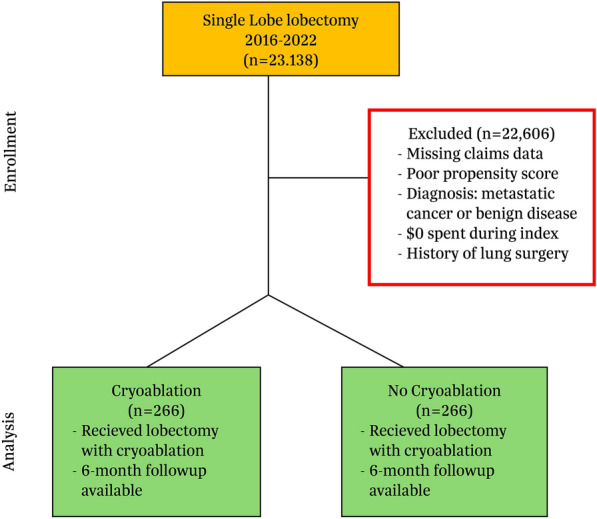
Results: From a cohort of 23,138 patients, 266 pairs with a mean age of 69 years were included. Matching variables included age, gender, lobe resected, and prior opioid use. Both groups had significant comorbidity history and prior opioid use; 66% (n = 175 both groups) underwent open lobectomy and 53% (n = 142 vs. 143) had the upper lobe resected. Cryoablation intervention was associated with 1.3 days reduced hospital stay (8.8 vs. 10.1 days, p = 0.31) and no difference in perioperative safety. After 90 days, postsurgery cryoablation patients had lower opioid prescription refills (27.3 vs. 36.9 morphine milligram equivalents, p = 0.03). Cryoablation patient costs trended less than non-cryoablation patients during index ($38,753 vs. $43,974, p = 0.10) and lower through 6 months (total costs, $65,703 vs. $74,304, p = 0.10). There was no difference in postsurgery resource use, but a smaller proportion of cryoablation patients had outpatient hospital visits (83.1%, N = 221 vs. 92.9%, n = 247, p < 0.01).
Conclusion: Cryoablation during lobectomy is safe and does not add incremental hospital costs. Clinical meaningful reductions in length of stay and postsurgery opioid use were observed with cryoablation intervention. The addition of cryoablation during surgery to reduce postoperative pain appears to be a cost-effective therapy.
期刊介绍:
Pain and Therapy is an international, open access, peer-reviewed, rapid publication journal dedicated to the publication of high-quality clinical (all phases), observational, real-world, and health outcomes research around the discovery, development, and use of pain therapies and pain-related devices. Studies relating to diagnosis, pharmacoeconomics, public health, quality of life, and patient care, management, and education are also encouraged.
Areas of focus include, but are not limited to, acute pain, cancer pain, chronic pain, headache and migraine, neuropathic pain, opioids, palliative care and pain ethics, peri- and post-operative pain as well as rheumatic pain and fibromyalgia.
The journal is of interest to a broad audience of pharmaceutical and healthcare professionals and publishes original research, reviews, case reports, trial protocols, short communications such as commentaries and editorials, and letters. The journal is read by a global audience and receives submissions from around the world. Pain and Therapy will consider all scientifically sound research be it positive, confirmatory or negative data. Submissions are welcomed whether they relate to an international and/or a country-specific audience, something that is crucially important when researchers are trying to target more specific patient populations. This inclusive approach allows the journal to assist in the dissemination of all scientifically and ethically sound research.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


