Ron T Gansevoort, David C Wheeler, Francisco Martínez Debén, Marijn Speeckaert, Dirk Thomas, Mario Berger, Stefan Klein, Frauke Friedrichs, Karen Paraschin, Roland E Schmieder
{"title":"可溶性鸟苷酸环化酶激活剂runcaciguat显著改善慢性肾病患者蛋白尿:一项随机安慰剂对照临床试验","authors":"Ron T Gansevoort, David C Wheeler, Francisco Martínez Debén, Marijn Speeckaert, Dirk Thomas, Mario Berger, Stefan Klein, Frauke Friedrichs, Karen Paraschin, Roland E Schmieder","doi":"10.1093/ndt/gfae261","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and hypothesis: </strong>In chronic kidney disease (CKD) the nitric oxide (NO)-soluble guanylate cyclase (sGC)-cyclic guanosine monophosphate (cGMP) pathway is impaired. Runcaciguat, an sGC activator, activates heme-free sGC, restoring cGMP production. This phase 2a trial studied the efficacy, safety, and tolerability of runcaciguat in CKD patients with or without sodium-glucose co-transporter-2 inhibitor (SGLT2i).</p><p><strong>Methods: </strong>Patients with CKD and established atherosclerotic cardiovascular disease or heart failure, plus type 2 diabetes (T2D) and/or hypertension, were enrolled. All were receiving stable maximum tolerated renin-angiotensin system inhibitors with or without SGLT2i. They were randomized 3:1 to runcaciguat once daily, titrated weekly (30-120 mg if tolerated), or placebo for 8 weeks. The primary efficacy endpoint was urine albumin-to-creatinine ratio (UACR) (average of post-randomization Days 22, 29, and 57 vs baseline). CONCORD was separately powered for CKD and T2D with stable SGLT2i comedication, CKD and T2D without SGLT2i, and non-diabetic CKD.</p><p><strong>Results: </strong>Of 243 patients randomized, 229 were included in the full analysis set (FAS) and 170 in the per-protocol set (PPS). In the PPS, UACR decreased by -45.2% versus placebo with runcaciguat in patients with CKD without SGLT2i (P < 0.001) and by -48.1% versus placebo in patients with CKD taking SGLT2i (P = 0.02) In the FAS, the relative reductions were -46.9% (P < 0.001) and -44.8% (P = 0.01), respectively. No significant difference was observed between patients with or without SGLT2i. In non-diabetic CKD, UACR was reduced versus baseline with runcaciguat, but the change was not statistically significant (P = 0.10). Serious treatment-emergent adverse events were reported in 7% of patients receiving runcaciguat and 8% receiving placebo.</p><p><strong>Conclusion: </strong>Runcaciguat improved albuminuria in patients with CKD, irrespective of concomitant SGLT2i. Runcaciguat was well tolerated. sGC activation may represent a novel kidney-protective treatment in CKD patients (funded by Bayer AG; ClinicalTrials.gov number, NCT04507061).</p>","PeriodicalId":19078,"journal":{"name":"Nephrology Dialysis Transplantation","volume":" ","pages":"1147-1160"},"PeriodicalIF":5.6000,"publicationDate":"2025-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12123308/pdf/","citationCount":"0","resultStr":"{\"title\":\"The soluble guanylate cyclase activator runcaciguat significantly improves albuminuria in patients with chronic kidney disease: a randomized placebo-controlled clinical trial.\",\"authors\":\"Ron T Gansevoort, David C Wheeler, Francisco Martínez Debén, Marijn Speeckaert, Dirk Thomas, Mario Berger, Stefan Klein, Frauke Friedrichs, Karen Paraschin, Roland E Schmieder\",\"doi\":\"10.1093/ndt/gfae261\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and hypothesis: </strong>In chronic kidney disease (CKD) the nitric oxide (NO)-soluble guanylate cyclase (sGC)-cyclic guanosine monophosphate (cGMP) pathway is impaired. Runcaciguat, an sGC activator, activates heme-free sGC, restoring cGMP production. This phase 2a trial studied the efficacy, safety, and tolerability of runcaciguat in CKD patients with or without sodium-glucose co-transporter-2 inhibitor (SGLT2i).</p><p><strong>Methods: </strong>Patients with CKD and established atherosclerotic cardiovascular disease or heart failure, plus type 2 diabetes (T2D) and/or hypertension, were enrolled. All were receiving stable maximum tolerated renin-angiotensin system inhibitors with or without SGLT2i. They were randomized 3:1 to runcaciguat once daily, titrated weekly (30-120 mg if tolerated), or placebo for 8 weeks. The primary efficacy endpoint was urine albumin-to-creatinine ratio (UACR) (average of post-randomization Days 22, 29, and 57 vs baseline). CONCORD was separately powered for CKD and T2D with stable SGLT2i comedication, CKD and T2D without SGLT2i, and non-diabetic CKD.</p><p><strong>Results: </strong>Of 243 patients randomized, 229 were included in the full analysis set (FAS) and 170 in the per-protocol set (PPS). In the PPS, UACR decreased by -45.2% versus placebo with runcaciguat in patients with CKD without SGLT2i (P < 0.001) and by -48.1% versus placebo in patients with CKD taking SGLT2i (P = 0.02) In the FAS, the relative reductions were -46.9% (P < 0.001) and -44.8% (P = 0.01), respectively. No significant difference was observed between patients with or without SGLT2i. In non-diabetic CKD, UACR was reduced versus baseline with runcaciguat, but the change was not statistically significant (P = 0.10). Serious treatment-emergent adverse events were reported in 7% of patients receiving runcaciguat and 8% receiving placebo.</p><p><strong>Conclusion: </strong>Runcaciguat improved albuminuria in patients with CKD, irrespective of concomitant SGLT2i. Runcaciguat was well tolerated. sGC activation may represent a novel kidney-protective treatment in CKD patients (funded by Bayer AG; ClinicalTrials.gov number, NCT04507061).</p>\",\"PeriodicalId\":19078,\"journal\":{\"name\":\"Nephrology Dialysis Transplantation\",\"volume\":\" \",\"pages\":\"1147-1160\"},\"PeriodicalIF\":5.6000,\"publicationDate\":\"2025-05-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12123308/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nephrology Dialysis Transplantation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ndt/gfae261\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"TRANSPLANTATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nephrology Dialysis Transplantation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ndt/gfae261","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
The soluble guanylate cyclase activator runcaciguat significantly improves albuminuria in patients with chronic kidney disease: a randomized placebo-controlled clinical trial.
Background and hypothesis: In chronic kidney disease (CKD) the nitric oxide (NO)-soluble guanylate cyclase (sGC)-cyclic guanosine monophosphate (cGMP) pathway is impaired. Runcaciguat, an sGC activator, activates heme-free sGC, restoring cGMP production. This phase 2a trial studied the efficacy, safety, and tolerability of runcaciguat in CKD patients with or without sodium-glucose co-transporter-2 inhibitor (SGLT2i).
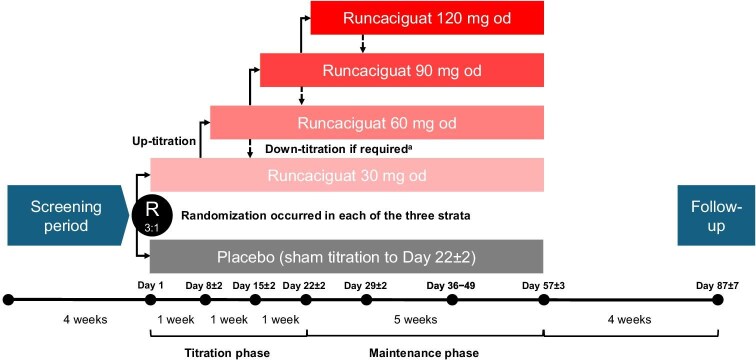
Methods: Patients with CKD and established atherosclerotic cardiovascular disease or heart failure, plus type 2 diabetes (T2D) and/or hypertension, were enrolled. All were receiving stable maximum tolerated renin-angiotensin system inhibitors with or without SGLT2i. They were randomized 3:1 to runcaciguat once daily, titrated weekly (30-120 mg if tolerated), or placebo for 8 weeks. The primary efficacy endpoint was urine albumin-to-creatinine ratio (UACR) (average of post-randomization Days 22, 29, and 57 vs baseline). CONCORD was separately powered for CKD and T2D with stable SGLT2i comedication, CKD and T2D without SGLT2i, and non-diabetic CKD.
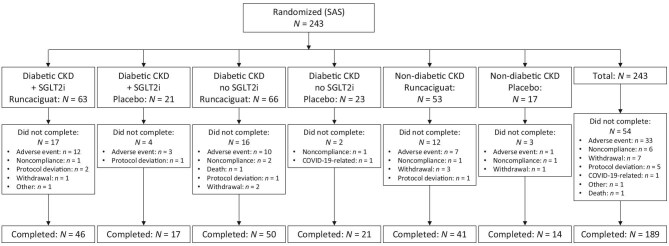
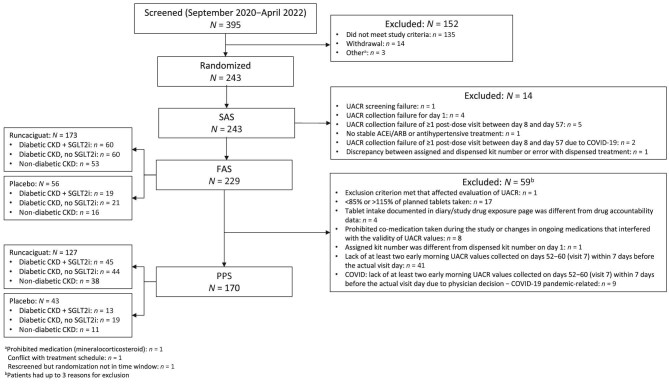
Results: Of 243 patients randomized, 229 were included in the full analysis set (FAS) and 170 in the per-protocol set (PPS). In the PPS, UACR decreased by -45.2% versus placebo with runcaciguat in patients with CKD without SGLT2i (P < 0.001) and by -48.1% versus placebo in patients with CKD taking SGLT2i (P = 0.02) In the FAS, the relative reductions were -46.9% (P < 0.001) and -44.8% (P = 0.01), respectively. No significant difference was observed between patients with or without SGLT2i. In non-diabetic CKD, UACR was reduced versus baseline with runcaciguat, but the change was not statistically significant (P = 0.10). Serious treatment-emergent adverse events were reported in 7% of patients receiving runcaciguat and 8% receiving placebo.
Conclusion: Runcaciguat improved albuminuria in patients with CKD, irrespective of concomitant SGLT2i. Runcaciguat was well tolerated. sGC activation may represent a novel kidney-protective treatment in CKD patients (funded by Bayer AG; ClinicalTrials.gov number, NCT04507061).
期刊介绍:
Nephrology Dialysis Transplantation (ndt) is the leading nephrology journal in Europe and renowned worldwide, devoted to original clinical and laboratory research in nephrology, dialysis and transplantation. ndt is an official journal of the [ERA-EDTA](http://www.era-edta.org/) (European Renal Association-European Dialysis and Transplant Association). Published monthly, the journal provides an essential resource for researchers and clinicians throughout the world. All research articles in this journal have undergone peer review.
Print ISSN: 0931-0509.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


