Jiayao Lei, Kate Cuschieri, Hasit Patel, Alexandra Lawrence, Katie Deats, Peter Sasieni, Anita W W Lim
{"title":"自采样的人类乳头瘤病毒基因型和周期阈值与高级别宫颈病变的风险:改良阶梯式楔形实施可行性试验的事后分析。","authors":"Jiayao Lei, Kate Cuschieri, Hasit Patel, Alexandra Lawrence, Katie Deats, Peter Sasieni, Anita W W Lim","doi":"10.1371/journal.pmed.1004494","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Human papillomavirus (HPV) testing of self-collected vaginal samples has potential to improve coverage of cervical screening programmes, but current guidelines mostly require those HPV positive on a self-sample to attend for routine screening.</p><p><strong>Methods and findings: </strong>A pragmatic modified stepped-wedge implementation feasibility trial was conducted at primary care practices in England. Individuals aged 25 to 64 years who were at least 6 months overdue for cervical screening could provide a self-collected sample. The primary outcomes included the monthly proportion of non-attenders screened, changes in coverage, and uptake within 90 days. Self-samples from 7,739 individuals were analysed using Roche Cobas 4800. Individuals with a positive self-sample were encouraged to attend clinical screening. In this post hoc study of the trial, we related the HPV type (HPV16, HPV18, or other high-risk type) and cycle threshold (Ct) value on the self-sample to the results of clinician-collected sample and cervical intraepithelial neoplasia grade 2 or worse (CIN2+). We wished to triage HPV-positive individuals to immediate colposcopy, clinician sampling, or 12-month recall depending on risk. A total of 1,001 women tested positive through self-samples, and 855 women who had both an HPV-positive self-sample and a subsequent clinician-sample were included in this study. Of these, 71 (8.3%) had CIN2+. Self-sample Ct values were highly predictive of HPV in the clinician sample. Combining HPV type and Ct value allowed stratification into 3 risk groups; 44/855 (5%) were high-risk of whom 43% (19/44, 95% confidence interval [29.7%, 57.8%]) had CIN2+. The majority (52.9%, 452/855) were low-risk, of whom 4% (18/452, 95% CI [2.5%, 6.2%]) had CIN2+. The main limitation of our study was the colposcopy assessment was restricted to individuals who had abnormal cytology after positive results of both self-sample and clinician-collected sample.</p><p><strong>Conclusions: </strong>HPV type and Ct value on HPV-positive self-samples may be used for triage. The difference in the risk of CIN2+ in these groups appears sufficient to justify differential clinical management. A prospective study employing such triage to evaluate laboratory workflow, acceptability, and follow-up procedure and to optimise clinical performance seems warranted.</p><p><strong>Trial registration: </strong>ISRCTN12759467.</p>","PeriodicalId":49008,"journal":{"name":"PLoS Medicine","volume":"21 12","pages":"e1004494"},"PeriodicalIF":9.9000,"publicationDate":"2024-12-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11637256/pdf/","citationCount":"0","resultStr":"{\"title\":\"Human papillomavirus genotype and cycle threshold value from self-samples and risk of high-grade cervical lesions: A post hoc analysis of a modified stepped-wedge implementation feasibility trial.\",\"authors\":\"Jiayao Lei, Kate Cuschieri, Hasit Patel, Alexandra Lawrence, Katie Deats, Peter Sasieni, Anita W W Lim\",\"doi\":\"10.1371/journal.pmed.1004494\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Human papillomavirus (HPV) testing of self-collected vaginal samples has potential to improve coverage of cervical screening programmes, but current guidelines mostly require those HPV positive on a self-sample to attend for routine screening.</p><p><strong>Methods and findings: </strong>A pragmatic modified stepped-wedge implementation feasibility trial was conducted at primary care practices in England. Individuals aged 25 to 64 years who were at least 6 months overdue for cervical screening could provide a self-collected sample. The primary outcomes included the monthly proportion of non-attenders screened, changes in coverage, and uptake within 90 days. Self-samples from 7,739 individuals were analysed using Roche Cobas 4800. Individuals with a positive self-sample were encouraged to attend clinical screening. In this post hoc study of the trial, we related the HPV type (HPV16, HPV18, or other high-risk type) and cycle threshold (Ct) value on the self-sample to the results of clinician-collected sample and cervical intraepithelial neoplasia grade 2 or worse (CIN2+). We wished to triage HPV-positive individuals to immediate colposcopy, clinician sampling, or 12-month recall depending on risk. A total of 1,001 women tested positive through self-samples, and 855 women who had both an HPV-positive self-sample and a subsequent clinician-sample were included in this study. Of these, 71 (8.3%) had CIN2+. Self-sample Ct values were highly predictive of HPV in the clinician sample. Combining HPV type and Ct value allowed stratification into 3 risk groups; 44/855 (5%) were high-risk of whom 43% (19/44, 95% confidence interval [29.7%, 57.8%]) had CIN2+. The majority (52.9%, 452/855) were low-risk, of whom 4% (18/452, 95% CI [2.5%, 6.2%]) had CIN2+. The main limitation of our study was the colposcopy assessment was restricted to individuals who had abnormal cytology after positive results of both self-sample and clinician-collected sample.</p><p><strong>Conclusions: </strong>HPV type and Ct value on HPV-positive self-samples may be used for triage. The difference in the risk of CIN2+ in these groups appears sufficient to justify differential clinical management. A prospective study employing such triage to evaluate laboratory workflow, acceptability, and follow-up procedure and to optimise clinical performance seems warranted.</p><p><strong>Trial registration: </strong>ISRCTN12759467.</p>\",\"PeriodicalId\":49008,\"journal\":{\"name\":\"PLoS Medicine\",\"volume\":\"21 12\",\"pages\":\"e1004494\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2024-12-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11637256/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pmed.1004494\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1004494","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Human papillomavirus genotype and cycle threshold value from self-samples and risk of high-grade cervical lesions: A post hoc analysis of a modified stepped-wedge implementation feasibility trial.
Background: Human papillomavirus (HPV) testing of self-collected vaginal samples has potential to improve coverage of cervical screening programmes, but current guidelines mostly require those HPV positive on a self-sample to attend for routine screening.
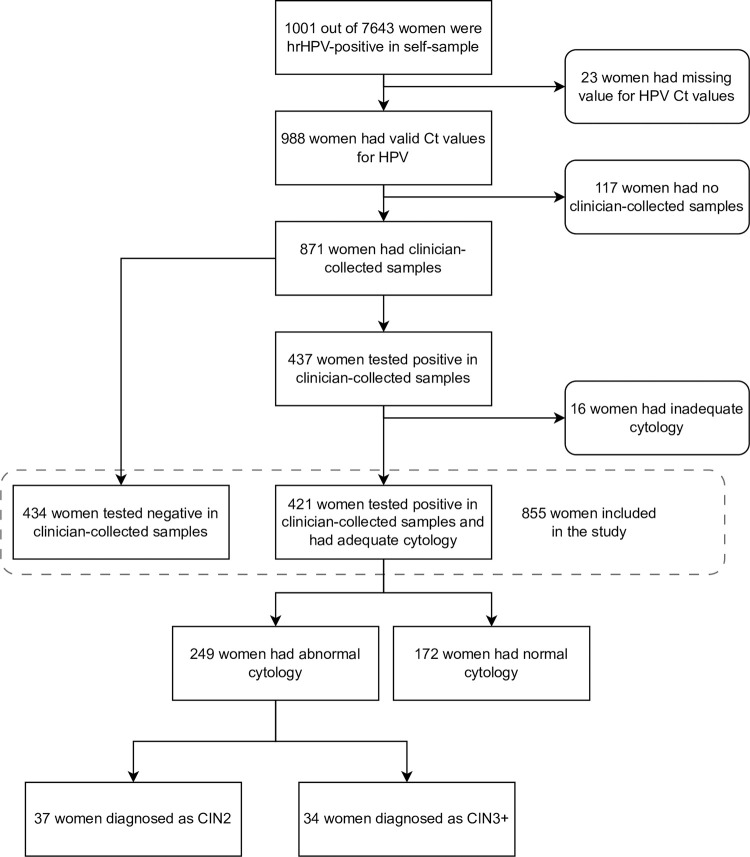
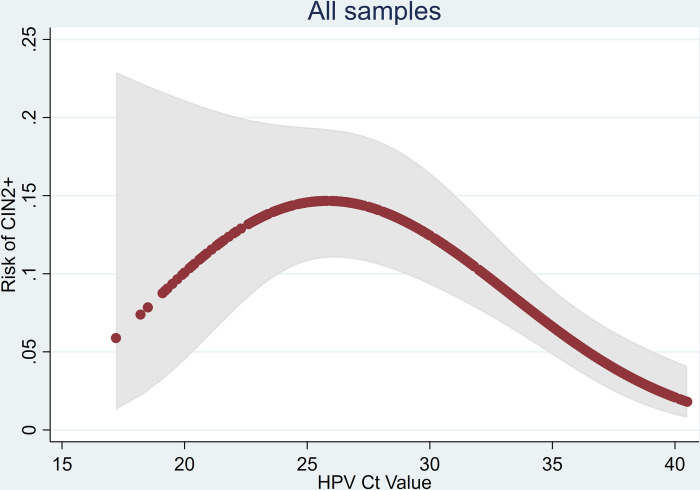
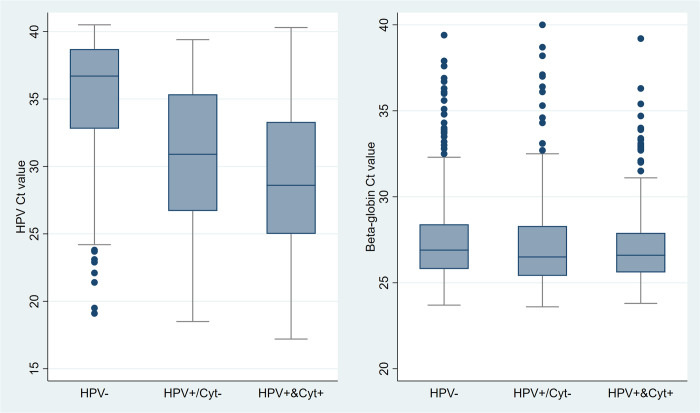
Methods and findings: A pragmatic modified stepped-wedge implementation feasibility trial was conducted at primary care practices in England. Individuals aged 25 to 64 years who were at least 6 months overdue for cervical screening could provide a self-collected sample. The primary outcomes included the monthly proportion of non-attenders screened, changes in coverage, and uptake within 90 days. Self-samples from 7,739 individuals were analysed using Roche Cobas 4800. Individuals with a positive self-sample were encouraged to attend clinical screening. In this post hoc study of the trial, we related the HPV type (HPV16, HPV18, or other high-risk type) and cycle threshold (Ct) value on the self-sample to the results of clinician-collected sample and cervical intraepithelial neoplasia grade 2 or worse (CIN2+). We wished to triage HPV-positive individuals to immediate colposcopy, clinician sampling, or 12-month recall depending on risk. A total of 1,001 women tested positive through self-samples, and 855 women who had both an HPV-positive self-sample and a subsequent clinician-sample were included in this study. Of these, 71 (8.3%) had CIN2+. Self-sample Ct values were highly predictive of HPV in the clinician sample. Combining HPV type and Ct value allowed stratification into 3 risk groups; 44/855 (5%) were high-risk of whom 43% (19/44, 95% confidence interval [29.7%, 57.8%]) had CIN2+. The majority (52.9%, 452/855) were low-risk, of whom 4% (18/452, 95% CI [2.5%, 6.2%]) had CIN2+. The main limitation of our study was the colposcopy assessment was restricted to individuals who had abnormal cytology after positive results of both self-sample and clinician-collected sample.
Conclusions: HPV type and Ct value on HPV-positive self-samples may be used for triage. The difference in the risk of CIN2+ in these groups appears sufficient to justify differential clinical management. A prospective study employing such triage to evaluate laboratory workflow, acceptability, and follow-up procedure and to optimise clinical performance seems warranted.
期刊介绍:
PLOS Medicine is a prominent platform for discussing and researching global health challenges. The journal covers a wide range of topics, including biomedical, environmental, social, and political factors affecting health. It prioritizes articles that contribute to clinical practice, health policy, or a better understanding of pathophysiology, ultimately aiming to improve health outcomes across different settings.
The journal is unwavering in its commitment to uphold the highest ethical standards in medical publishing. This includes actively managing and disclosing any conflicts of interest related to reporting, reviewing, and publishing. PLOS Medicine promotes transparency in the entire review and publication process. The journal also encourages data sharing and encourages the reuse of published work. Additionally, authors retain copyright for their work, and the publication is made accessible through Open Access with no restrictions on availability and dissemination.
PLOS Medicine takes measures to avoid conflicts of interest associated with advertising drugs and medical devices or engaging in the exclusive sale of reprints.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


