Mark H Wilcox, Dave Heaton, Aruni Mulgirigama, Ashish V Joshi, Viktor Chirikov, Daniel C Gibbons, David Webb, Xiaocong L Marston, Myriam Na Alexander, Fanny S Mitrani-Gold
{"title":"英格兰无并发症尿路感染的治疗模式和负担。","authors":"Mark H Wilcox, Dave Heaton, Aruni Mulgirigama, Ashish V Joshi, Viktor Chirikov, Daniel C Gibbons, David Webb, Xiaocong L Marston, Myriam Na Alexander, Fanny S Mitrani-Gold","doi":"10.3399/BJGPO.2024.0214","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Uncomplicated urinary tract infections (uUTIs) are common bacterial infections.</p><p><strong>Aim: </strong>To evaluate the burden of uUTI in England for 1) potential determinants of disease progression; 2) extent and impact of antimicrobial prescribing non-concordant with treatment guidelines; and 3) healthcare burden and economic costs.</p><p><strong>Design & setting: </strong>Retrospective cohort study utilising patient data (January 2017-February 2020) from the Clinical Practice Research Datalink (CPRD) linked to English Hospital Episode Statistics.</p><p><strong>Method: </strong>Female patients aged ≥12 years with a new uUTI between 2018 and 2019, ≥14 months' continuous CPRD enrolment (≥12 months baseline, ≥2 months follow-up), and ≥1 oral antibiotic prescription ±5 days of uUTI diagnosis were included. Baseline characteristics were described in patients with or without disease progression (hospitalisation for acute pyelonephritis, bacteraemia, or sepsis). Treatment non-concordance with current English guidelines was assessed. Burden (all-cause and urinary tract infection-related healthcare resource use [HCRU] and costs) was evaluated in a 1:1 age and comorbidity-matched uUTI-free cohort.</p><p><strong>Results: </strong>Of 120 519 patients, 207 (0.2%) had disease progression requiring hospitalisation (during index uUTI episode); determinants included older age, index uUTI home consultation, prior hospitalisation, and medications prescribed for comorbid conditions in the prior 12 months (<i>British National Formulary</i> classes: cardiovascular system, eye, and other drugs and preparations). Non-concordant treatment was observed in 43.5% of patients. All-cause HCRU burden and costs were significantly higher in patients with uUTI versus age and comorbidity-matched controls (<i>P</i><0.001) at 28 days (£160.06 versus £37.63) and in the 12-month follow-up (£1206.77 versus £460.97).</p><p><strong>Conclusion: </strong>All-cause HCRU burden and costs were significantly higher in patients with uUTI versus matched controls (<i>P</i><0.001). Hospitalisation for acute pyelonephritis, bacteraemia, or sepsis following uUTI was uncommon.</p>","PeriodicalId":36541,"journal":{"name":"BJGP Open","volume":" ","pages":""},"PeriodicalIF":2.0000,"publicationDate":"2025-07-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421281/pdf/","citationCount":"0","resultStr":"{\"title\":\"Treatment patterns and burden of uncomplicated urinary tract infection in England: a retrospective cohort study.\",\"authors\":\"Mark H Wilcox, Dave Heaton, Aruni Mulgirigama, Ashish V Joshi, Viktor Chirikov, Daniel C Gibbons, David Webb, Xiaocong L Marston, Myriam Na Alexander, Fanny S Mitrani-Gold\",\"doi\":\"10.3399/BJGPO.2024.0214\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Uncomplicated urinary tract infections (uUTIs) are common bacterial infections.</p><p><strong>Aim: </strong>To evaluate the burden of uUTI in England for 1) potential determinants of disease progression; 2) extent and impact of antimicrobial prescribing non-concordant with treatment guidelines; and 3) healthcare burden and economic costs.</p><p><strong>Design & setting: </strong>Retrospective cohort study utilising patient data (January 2017-February 2020) from the Clinical Practice Research Datalink (CPRD) linked to English Hospital Episode Statistics.</p><p><strong>Method: </strong>Female patients aged ≥12 years with a new uUTI between 2018 and 2019, ≥14 months' continuous CPRD enrolment (≥12 months baseline, ≥2 months follow-up), and ≥1 oral antibiotic prescription ±5 days of uUTI diagnosis were included. Baseline characteristics were described in patients with or without disease progression (hospitalisation for acute pyelonephritis, bacteraemia, or sepsis). Treatment non-concordance with current English guidelines was assessed. Burden (all-cause and urinary tract infection-related healthcare resource use [HCRU] and costs) was evaluated in a 1:1 age and comorbidity-matched uUTI-free cohort.</p><p><strong>Results: </strong>Of 120 519 patients, 207 (0.2%) had disease progression requiring hospitalisation (during index uUTI episode); determinants included older age, index uUTI home consultation, prior hospitalisation, and medications prescribed for comorbid conditions in the prior 12 months (<i>British National Formulary</i> classes: cardiovascular system, eye, and other drugs and preparations). Non-concordant treatment was observed in 43.5% of patients. All-cause HCRU burden and costs were significantly higher in patients with uUTI versus age and comorbidity-matched controls (<i>P</i><0.001) at 28 days (£160.06 versus £37.63) and in the 12-month follow-up (£1206.77 versus £460.97).</p><p><strong>Conclusion: </strong>All-cause HCRU burden and costs were significantly higher in patients with uUTI versus matched controls (<i>P</i><0.001). Hospitalisation for acute pyelonephritis, bacteraemia, or sepsis following uUTI was uncommon.</p>\",\"PeriodicalId\":36541,\"journal\":{\"name\":\"BJGP Open\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-07-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421281/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BJGP Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3399/BJGPO.2024.0214\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"Q2\",\"JCRName\":\"PRIMARY HEALTH CARE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJGP Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3399/BJGPO.2024.0214","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
Treatment patterns and burden of uncomplicated urinary tract infection in England: a retrospective cohort study.
Background: Uncomplicated urinary tract infections (uUTIs) are common bacterial infections.
Aim: To evaluate the burden of uUTI in England for 1) potential determinants of disease progression; 2) extent and impact of antimicrobial prescribing non-concordant with treatment guidelines; and 3) healthcare burden and economic costs.
Design & setting: Retrospective cohort study utilising patient data (January 2017-February 2020) from the Clinical Practice Research Datalink (CPRD) linked to English Hospital Episode Statistics.
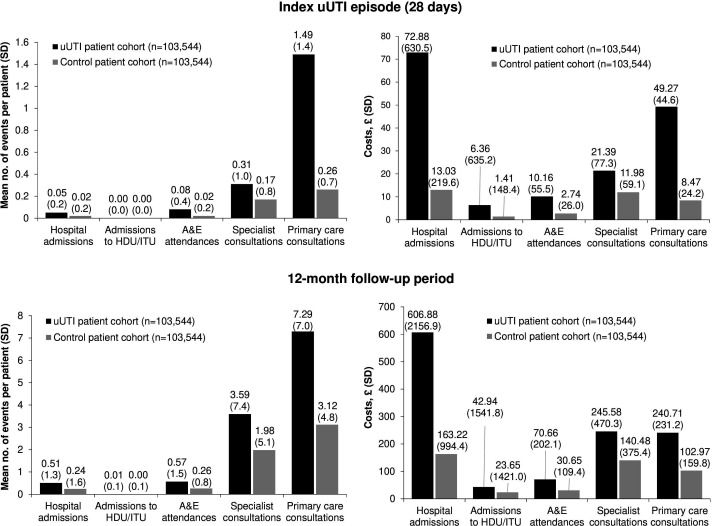
Method: Female patients aged ≥12 years with a new uUTI between 2018 and 2019, ≥14 months' continuous CPRD enrolment (≥12 months baseline, ≥2 months follow-up), and ≥1 oral antibiotic prescription ±5 days of uUTI diagnosis were included. Baseline characteristics were described in patients with or without disease progression (hospitalisation for acute pyelonephritis, bacteraemia, or sepsis). Treatment non-concordance with current English guidelines was assessed. Burden (all-cause and urinary tract infection-related healthcare resource use [HCRU] and costs) was evaluated in a 1:1 age and comorbidity-matched uUTI-free cohort.
Results: Of 120 519 patients, 207 (0.2%) had disease progression requiring hospitalisation (during index uUTI episode); determinants included older age, index uUTI home consultation, prior hospitalisation, and medications prescribed for comorbid conditions in the prior 12 months (British National Formulary classes: cardiovascular system, eye, and other drugs and preparations). Non-concordant treatment was observed in 43.5% of patients. All-cause HCRU burden and costs were significantly higher in patients with uUTI versus age and comorbidity-matched controls (P<0.001) at 28 days (£160.06 versus £37.63) and in the 12-month follow-up (£1206.77 versus £460.97).
Conclusion: All-cause HCRU burden and costs were significantly higher in patients with uUTI versus matched controls (P<0.001). Hospitalisation for acute pyelonephritis, bacteraemia, or sepsis following uUTI was uncommon.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


