Jing Yuan Tan, Jeffrey Kim Siang Quek, Ming Lee, Lai Peng Chan, William Ying Khee Hwang, Francesca Wei Inng Lim, Aloysius Yew Leng Ho, Yeh Ching Linn, Yeow Tee Goh, Hein Than
{"title":"慢性移植物抗宿主病多肌炎影响呼吸和躯干肌的可能病例-一个全面的诊断方法。","authors":"Jing Yuan Tan, Jeffrey Kim Siang Quek, Ming Lee, Lai Peng Chan, William Ying Khee Hwang, Francesca Wei Inng Lim, Aloysius Yew Leng Ho, Yeh Ching Linn, Yeow Tee Goh, Hein Than","doi":"10.31547/bct-2023-040","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Muscle involvement, termed polymyositis, is an uncommon manifestation of graft-versus-host disease (GvHD) in which the upper and lower limbs are commonly affected. However, respiratory failure due to diaphragmatic weakness has rarely been reported. Diagnosis is usually based on a combination of elevated muscle enzyme levels in the blood, neurophysiological studies, and muscle biopsies.</p><p><strong>Case report: </strong>A 23-year-old man who presented with Philadelphia chromosome (Ph)-positive chronic myeloid leukemia in myeloid blast crisis, underwent HLA-matched sibling (sister) hematopoietic stem cell transplantation. Six months post-transplant, he experienced bilateral arm pain and weakness, with an inability to raise his limbs against gravity. He was also unable to sit erect, and was dyspneic and hypoxic, thus requiring oxygen supplementation. Serum muscle enzyme levels were found to be markedly elevated. Magnetic resonance imaging showed a patchy hyperintense T2-weighted signal and enhancement in the muscle groups of the limbs, as well as in the psoas and erector spinae muscles. The electromyogram results were consistent with those of inflammatory myopathy. Muscle biopsy revealed extensive necrotizing myositis with extensive lymphocyte infiltration throughout the muscle fascicle. Additionally, fluorescence in situ hybridization (FISH) analysis demonstrated that 30% of the nuclei scored were in the muscle fibers of recipient XY origin, and 70% were in T-lymphocytes of donor XX origin. GvHD polymyositis was diagnosed, and the patient responded well to corticosteroids and extracorporeal photopheresis.</p><p><strong>Conclusion: </strong>GvHD polymyositis can affect various muscle groups and results in various clinical presentations. In our case, truncal involvement resulting in an inability to sit erect was a unique presentation. Prompt diagnosis is important, and we have highlighted a comprehensive multimodal approach, including the potential use of FISH analysis, to aid in diagnosis.</p>","PeriodicalId":72423,"journal":{"name":"Blood cell therapy","volume":"7 4","pages":"106-110"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11620988/pdf/","citationCount":"0","resultStr":"{\"title\":\"A likely case of chronic graft-versus-host disease polymyositis affecting respiratory and truncal muscles - a comprehensive diagnostic approach.\",\"authors\":\"Jing Yuan Tan, Jeffrey Kim Siang Quek, Ming Lee, Lai Peng Chan, William Ying Khee Hwang, Francesca Wei Inng Lim, Aloysius Yew Leng Ho, Yeh Ching Linn, Yeow Tee Goh, Hein Than\",\"doi\":\"10.31547/bct-2023-040\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Muscle involvement, termed polymyositis, is an uncommon manifestation of graft-versus-host disease (GvHD) in which the upper and lower limbs are commonly affected. However, respiratory failure due to diaphragmatic weakness has rarely been reported. Diagnosis is usually based on a combination of elevated muscle enzyme levels in the blood, neurophysiological studies, and muscle biopsies.</p><p><strong>Case report: </strong>A 23-year-old man who presented with Philadelphia chromosome (Ph)-positive chronic myeloid leukemia in myeloid blast crisis, underwent HLA-matched sibling (sister) hematopoietic stem cell transplantation. Six months post-transplant, he experienced bilateral arm pain and weakness, with an inability to raise his limbs against gravity. He was also unable to sit erect, and was dyspneic and hypoxic, thus requiring oxygen supplementation. Serum muscle enzyme levels were found to be markedly elevated. Magnetic resonance imaging showed a patchy hyperintense T2-weighted signal and enhancement in the muscle groups of the limbs, as well as in the psoas and erector spinae muscles. The electromyogram results were consistent with those of inflammatory myopathy. Muscle biopsy revealed extensive necrotizing myositis with extensive lymphocyte infiltration throughout the muscle fascicle. Additionally, fluorescence in situ hybridization (FISH) analysis demonstrated that 30% of the nuclei scored were in the muscle fibers of recipient XY origin, and 70% were in T-lymphocytes of donor XX origin. GvHD polymyositis was diagnosed, and the patient responded well to corticosteroids and extracorporeal photopheresis.</p><p><strong>Conclusion: </strong>GvHD polymyositis can affect various muscle groups and results in various clinical presentations. In our case, truncal involvement resulting in an inability to sit erect was a unique presentation. Prompt diagnosis is important, and we have highlighted a comprehensive multimodal approach, including the potential use of FISH analysis, to aid in diagnosis.</p>\",\"PeriodicalId\":72423,\"journal\":{\"name\":\"Blood cell therapy\",\"volume\":\"7 4\",\"pages\":\"106-110\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-09-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11620988/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Blood cell therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31547/bct-2023-040\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/25 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood cell therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31547/bct-2023-040","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/25 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
A likely case of chronic graft-versus-host disease polymyositis affecting respiratory and truncal muscles - a comprehensive diagnostic approach.
Background: Muscle involvement, termed polymyositis, is an uncommon manifestation of graft-versus-host disease (GvHD) in which the upper and lower limbs are commonly affected. However, respiratory failure due to diaphragmatic weakness has rarely been reported. Diagnosis is usually based on a combination of elevated muscle enzyme levels in the blood, neurophysiological studies, and muscle biopsies.
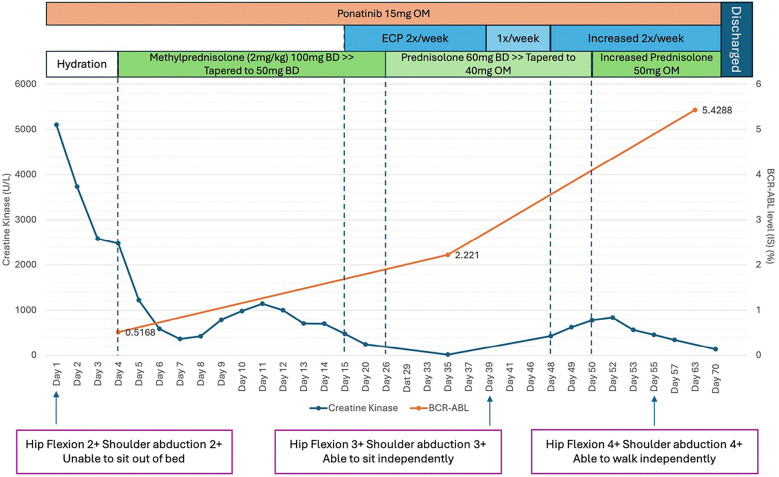
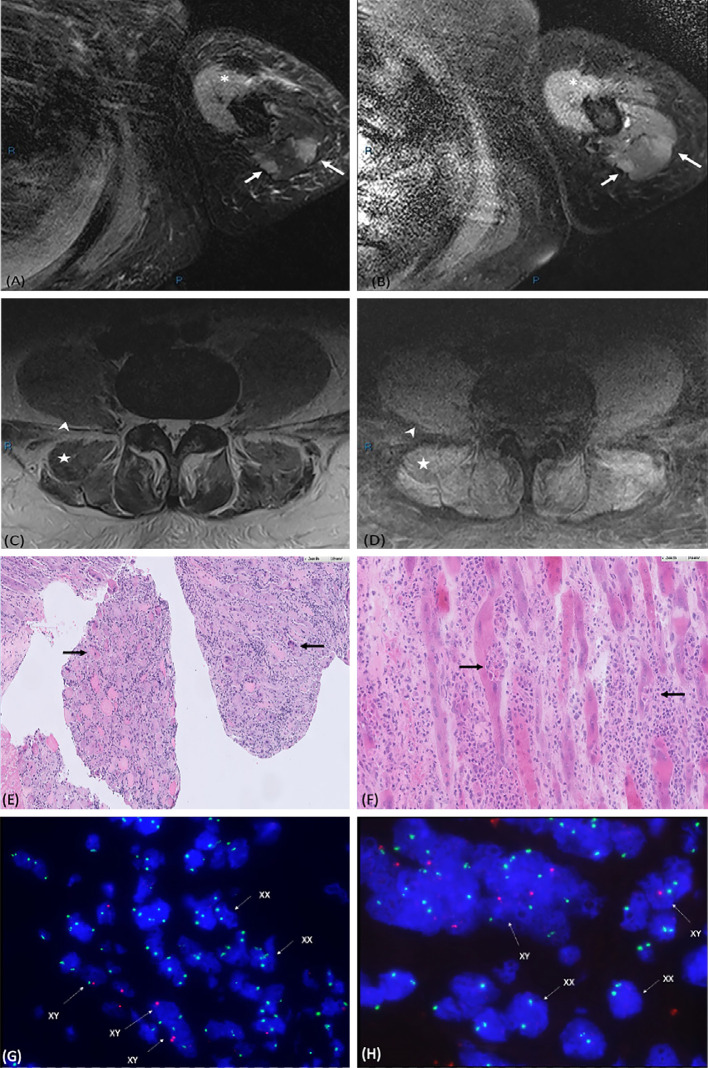
Case report: A 23-year-old man who presented with Philadelphia chromosome (Ph)-positive chronic myeloid leukemia in myeloid blast crisis, underwent HLA-matched sibling (sister) hematopoietic stem cell transplantation. Six months post-transplant, he experienced bilateral arm pain and weakness, with an inability to raise his limbs against gravity. He was also unable to sit erect, and was dyspneic and hypoxic, thus requiring oxygen supplementation. Serum muscle enzyme levels were found to be markedly elevated. Magnetic resonance imaging showed a patchy hyperintense T2-weighted signal and enhancement in the muscle groups of the limbs, as well as in the psoas and erector spinae muscles. The electromyogram results were consistent with those of inflammatory myopathy. Muscle biopsy revealed extensive necrotizing myositis with extensive lymphocyte infiltration throughout the muscle fascicle. Additionally, fluorescence in situ hybridization (FISH) analysis demonstrated that 30% of the nuclei scored were in the muscle fibers of recipient XY origin, and 70% were in T-lymphocytes of donor XX origin. GvHD polymyositis was diagnosed, and the patient responded well to corticosteroids and extracorporeal photopheresis.
Conclusion: GvHD polymyositis can affect various muscle groups and results in various clinical presentations. In our case, truncal involvement resulting in an inability to sit erect was a unique presentation. Prompt diagnosis is important, and we have highlighted a comprehensive multimodal approach, including the potential use of FISH analysis, to aid in diagnosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


