Pavel Goriacko, Ladan Golestaneh, Katherine E Di Palo
{"title":"急性高钾血症在急诊科辅助胰岛素治疗的回顾性研究。","authors":"Pavel Goriacko, Ladan Golestaneh, Katherine E Di Palo","doi":"10.2147/OAEM.S478693","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To investigate the clinical utility of administering patiromer as an adjunct to insulin for potassium reduction in patients presenting to the emergency department (ED) with hyperkalemia.</p><p><strong>Methods: </strong> This retrospective cohort study used electronic health record data to identify adults treated with at least one intravenous dose of regular insulin for hyperkalemia within the ED. Patients who were administered patiromer within one hour before or after their insulin dose were categorized as the intervention group. Matching was performed at a 1:1 ratio. The primary outcome, mean change in potassium from baseline to the latest value within the 4-12 hour interval, was compared. Secondary outcomes included net clinical benefit, defined as the mean difference in the number of potassium-lowering interventions minus the change in potassium.</p><p><strong>Results: </strong>The final analysis included 133 patients treated with patiromer plus insulin and 133 patients treated with insulin alone. Participants had a mean age of 71 years; 43% were female, 31% self-identified as Black, and 38% self-identified as Latinx. No significant changes were observed in potassium from baseline (mean levels 6.2 mEq/L in each group) to the 4-12 hour time frame (patiromer: -0.90 mEq/L, n=78 vs insulin-only: -0.98 mEq/L, n=81; p = 0.51). The calculated net clinical benefit of potassium reduction was -0.25 in favor of the patiromer plus insulin group; however, this difference did not reach statistical significance. In the subgroup of eGFR >30 mL/min, patiromer group received numerically less potassium-lowering interventions (0.63 vs 1.12, p = 0.057).</p><p><strong>Conclusion: </strong>In this study of patients with acute hyperkalemia in the ED setting, concurrent administration of patiromer did not result in more sustained potassium reduction compared to insulin alone in the overall cohort. The trend in favor of adjunct patiromer in the subgroup with adequate renal function warrants further investigation.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"16 ","pages":"305-312"},"PeriodicalIF":1.5000,"publicationDate":"2024-12-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11626971/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Retrospective Study of Patiromer as Adjunct to Insulin Therapy for Acute Hyperkalemia in the Emergency Department.\",\"authors\":\"Pavel Goriacko, Ladan Golestaneh, Katherine E Di Palo\",\"doi\":\"10.2147/OAEM.S478693\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To investigate the clinical utility of administering patiromer as an adjunct to insulin for potassium reduction in patients presenting to the emergency department (ED) with hyperkalemia.</p><p><strong>Methods: </strong> This retrospective cohort study used electronic health record data to identify adults treated with at least one intravenous dose of regular insulin for hyperkalemia within the ED. Patients who were administered patiromer within one hour before or after their insulin dose were categorized as the intervention group. Matching was performed at a 1:1 ratio. The primary outcome, mean change in potassium from baseline to the latest value within the 4-12 hour interval, was compared. Secondary outcomes included net clinical benefit, defined as the mean difference in the number of potassium-lowering interventions minus the change in potassium.</p><p><strong>Results: </strong>The final analysis included 133 patients treated with patiromer plus insulin and 133 patients treated with insulin alone. Participants had a mean age of 71 years; 43% were female, 31% self-identified as Black, and 38% self-identified as Latinx. No significant changes were observed in potassium from baseline (mean levels 6.2 mEq/L in each group) to the 4-12 hour time frame (patiromer: -0.90 mEq/L, n=78 vs insulin-only: -0.98 mEq/L, n=81; p = 0.51). The calculated net clinical benefit of potassium reduction was -0.25 in favor of the patiromer plus insulin group; however, this difference did not reach statistical significance. In the subgroup of eGFR >30 mL/min, patiromer group received numerically less potassium-lowering interventions (0.63 vs 1.12, p = 0.057).</p><p><strong>Conclusion: </strong>In this study of patients with acute hyperkalemia in the ED setting, concurrent administration of patiromer did not result in more sustained potassium reduction compared to insulin alone in the overall cohort. The trend in favor of adjunct patiromer in the subgroup with adequate renal function warrants further investigation.</p>\",\"PeriodicalId\":45096,\"journal\":{\"name\":\"Open Access Emergency Medicine\",\"volume\":\"16 \",\"pages\":\"305-312\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2024-12-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11626971/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Access Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OAEM.S478693\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S478693","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
目的:探讨在急诊科(ED)高钾血症患者中应用帕利莫辅助胰岛素治疗降钾的临床应用价值。方法:这项回顾性队列研究使用电子健康记录数据来识别在急诊科内接受至少一次静脉注射常规胰岛素治疗的高钾血症的成年人。在胰岛素剂量之前或之后一小时内给予胰岛素治疗的患者被归类为干预组。匹配以1:1的比例进行。比较主要结局,4-12小时间隔内钾从基线到最新值的平均变化。次要结果包括净临床获益,定义为降钾干预次数的平均差异减去钾的变化。结果:最终分析包括133例联合胰岛素治疗患者和133例单独胰岛素治疗患者。参与者的平均年龄为71岁;43%为女性,31%自认为是黑人,38%自认为是拉丁裔。从基线(每组平均水平6.2 mEq/L)到4-12小时时间范围内,钾未观察到显著变化(对照组:-0.90 mEq/L, n=78 vs胰岛素组:-0.98 mEq/L, n=81;P = 0.51)。减少钾的计算净临床效益为-0.25,有利于帕特罗默加胰岛素组;然而,这种差异没有达到统计学意义。在eGFR低于30 mL/min亚组中,患者组接受的降钾干预数量较少(0.63 vs 1.12, p = 0.057)。结论:在这项对急症患者急性高钾血症的研究中,在整个队列中,与单独使用胰岛素相比,同时使用帕利莫并没有导致更持久的钾减少。在肾功能良好的亚组中,辅助用药的趋势值得进一步研究。
A Retrospective Study of Patiromer as Adjunct to Insulin Therapy for Acute Hyperkalemia in the Emergency Department.
Objective: To investigate the clinical utility of administering patiromer as an adjunct to insulin for potassium reduction in patients presenting to the emergency department (ED) with hyperkalemia.
Methods: This retrospective cohort study used electronic health record data to identify adults treated with at least one intravenous dose of regular insulin for hyperkalemia within the ED. Patients who were administered patiromer within one hour before or after their insulin dose were categorized as the intervention group. Matching was performed at a 1:1 ratio. The primary outcome, mean change in potassium from baseline to the latest value within the 4-12 hour interval, was compared. Secondary outcomes included net clinical benefit, defined as the mean difference in the number of potassium-lowering interventions minus the change in potassium.
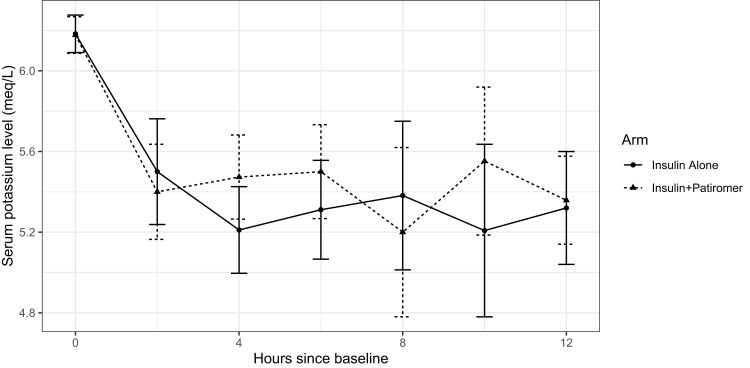
Results: The final analysis included 133 patients treated with patiromer plus insulin and 133 patients treated with insulin alone. Participants had a mean age of 71 years; 43% were female, 31% self-identified as Black, and 38% self-identified as Latinx. No significant changes were observed in potassium from baseline (mean levels 6.2 mEq/L in each group) to the 4-12 hour time frame (patiromer: -0.90 mEq/L, n=78 vs insulin-only: -0.98 mEq/L, n=81; p = 0.51). The calculated net clinical benefit of potassium reduction was -0.25 in favor of the patiromer plus insulin group; however, this difference did not reach statistical significance. In the subgroup of eGFR >30 mL/min, patiromer group received numerically less potassium-lowering interventions (0.63 vs 1.12, p = 0.057).
Conclusion: In this study of patients with acute hyperkalemia in the ED setting, concurrent administration of patiromer did not result in more sustained potassium reduction compared to insulin alone in the overall cohort. The trend in favor of adjunct patiromer in the subgroup with adequate renal function warrants further investigation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


