{"title":"甘油三酯沉积性心肌病血液透析患者的肉毒碱给药和123I-BMIPP洗脱率","authors":"Ken-Ichi Hirano, Keita Kodama, Hideyuki Miyauchi, Yasuyuki Nagasawa, Yusuke Nakano, Masaki Matsunaga, Tetsuya Amano, Kenichi Nakajima","doi":"10.17996/anc.23-00014","DOIUrl":null,"url":null,"abstract":"<p><p>Triglyceride deposit cardiomyovasculopathy (TGCV) is an emerging rare heart disease with high mortality, characterized by defective intracellular lipolysis of triglycerides (TG). We developed diagnostic criteria for TGCV, in which low washout rate of BMIPP (BMIPP-WR) is a key factor. The working group of the Japan Society of Nuclear Cardiology recently published practice recommendations for measuring BMIPP-WR. We reported that hemodialysis (HD) patients with TGCV exhibited a markedly higher cardiovascular risk than those without TGCV. Secondary carnitine deficiency is common in patients undergoing HD, as carnitine is removed from the circulation. However, clinical evidence linking carnitine levels to BMIPP-WR is limited. Here we report the effect of L-carnitine administration on the BMIPP-WR in 9 chronic HD patients with TGCV in a retrospective cohort. The mean age at TGCV diagnosis was 59 years. Following standard doses of oral L-carnitine administration, plasma free carnitine levels significantly increased. However, BMIPP-WR was not changed. In normal condition, most BMIPP taken up were esterified/incorporated into TG pool, hydrolyzed by intracellular lipases, and then transported by carnitine shuttle to mitochondria. In TGCV, intracellular TG lipolysis is defective. During the intracellular metabolism of BMIPP, carnitine shuttling occurs downstream of TG lipolysis. Therefore, even when carnitine levels were increased, BMIPP-WR did not change in patients with TGCV who underwent chronic HD. A phase IIb/III clinical trial for TGCV, is underway (jRCT2051210177). Increased awareness of the disease concept of TGCV, along with its diagnostic principles and procedures using BMIPP scintigraphy, is warranted.</p>","PeriodicalId":72228,"journal":{"name":"Annals of nuclear cardiology","volume":"10 1","pages":"38-42"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11612398/pdf/","citationCount":"0","resultStr":"{\"title\":\"Carnitine Administration and <sup>123</sup>I-BMIPP Washout Rate in Hemodialysis Patients with Triglyceride Deposit Cardiomyovasculopathy.\",\"authors\":\"Ken-Ichi Hirano, Keita Kodama, Hideyuki Miyauchi, Yasuyuki Nagasawa, Yusuke Nakano, Masaki Matsunaga, Tetsuya Amano, Kenichi Nakajima\",\"doi\":\"10.17996/anc.23-00014\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Triglyceride deposit cardiomyovasculopathy (TGCV) is an emerging rare heart disease with high mortality, characterized by defective intracellular lipolysis of triglycerides (TG). We developed diagnostic criteria for TGCV, in which low washout rate of BMIPP (BMIPP-WR) is a key factor. The working group of the Japan Society of Nuclear Cardiology recently published practice recommendations for measuring BMIPP-WR. We reported that hemodialysis (HD) patients with TGCV exhibited a markedly higher cardiovascular risk than those without TGCV. Secondary carnitine deficiency is common in patients undergoing HD, as carnitine is removed from the circulation. However, clinical evidence linking carnitine levels to BMIPP-WR is limited. Here we report the effect of L-carnitine administration on the BMIPP-WR in 9 chronic HD patients with TGCV in a retrospective cohort. The mean age at TGCV diagnosis was 59 years. Following standard doses of oral L-carnitine administration, plasma free carnitine levels significantly increased. However, BMIPP-WR was not changed. In normal condition, most BMIPP taken up were esterified/incorporated into TG pool, hydrolyzed by intracellular lipases, and then transported by carnitine shuttle to mitochondria. In TGCV, intracellular TG lipolysis is defective. During the intracellular metabolism of BMIPP, carnitine shuttling occurs downstream of TG lipolysis. Therefore, even when carnitine levels were increased, BMIPP-WR did not change in patients with TGCV who underwent chronic HD. A phase IIb/III clinical trial for TGCV, is underway (jRCT2051210177). Increased awareness of the disease concept of TGCV, along with its diagnostic principles and procedures using BMIPP scintigraphy, is warranted.</p>\",\"PeriodicalId\":72228,\"journal\":{\"name\":\"Annals of nuclear cardiology\",\"volume\":\"10 1\",\"pages\":\"38-42\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11612398/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of nuclear cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.17996/anc.23-00014\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/31 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of nuclear cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17996/anc.23-00014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Carnitine Administration and 123I-BMIPP Washout Rate in Hemodialysis Patients with Triglyceride Deposit Cardiomyovasculopathy.
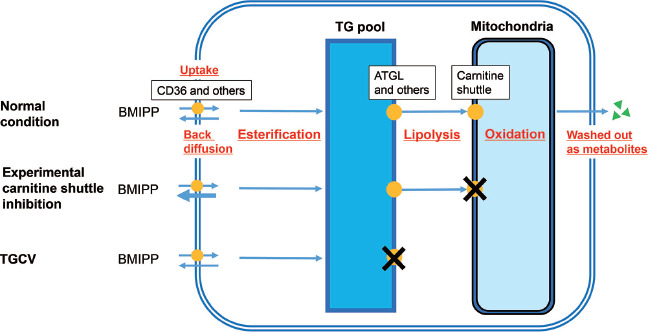
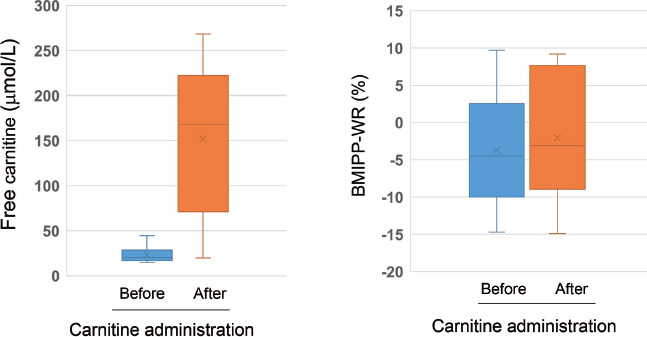
Triglyceride deposit cardiomyovasculopathy (TGCV) is an emerging rare heart disease with high mortality, characterized by defective intracellular lipolysis of triglycerides (TG). We developed diagnostic criteria for TGCV, in which low washout rate of BMIPP (BMIPP-WR) is a key factor. The working group of the Japan Society of Nuclear Cardiology recently published practice recommendations for measuring BMIPP-WR. We reported that hemodialysis (HD) patients with TGCV exhibited a markedly higher cardiovascular risk than those without TGCV. Secondary carnitine deficiency is common in patients undergoing HD, as carnitine is removed from the circulation. However, clinical evidence linking carnitine levels to BMIPP-WR is limited. Here we report the effect of L-carnitine administration on the BMIPP-WR in 9 chronic HD patients with TGCV in a retrospective cohort. The mean age at TGCV diagnosis was 59 years. Following standard doses of oral L-carnitine administration, plasma free carnitine levels significantly increased. However, BMIPP-WR was not changed. In normal condition, most BMIPP taken up were esterified/incorporated into TG pool, hydrolyzed by intracellular lipases, and then transported by carnitine shuttle to mitochondria. In TGCV, intracellular TG lipolysis is defective. During the intracellular metabolism of BMIPP, carnitine shuttling occurs downstream of TG lipolysis. Therefore, even when carnitine levels were increased, BMIPP-WR did not change in patients with TGCV who underwent chronic HD. A phase IIb/III clinical trial for TGCV, is underway (jRCT2051210177). Increased awareness of the disease concept of TGCV, along with its diagnostic principles and procedures using BMIPP scintigraphy, is warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


