Patrick Gahr, Manuel Matthis, Lennart Schleese, Dagmar-C Fischer, Thomas Mittlmeier
{"title":"在不稳定踝关节骨折的治疗中,与标准管状钢板相比,现代解剖锁定钢板与术后伤口并发症和计划外手术翻修相关:一项595例患者的比较队列研究。","authors":"Patrick Gahr, Manuel Matthis, Lennart Schleese, Dagmar-C Fischer, Thomas Mittlmeier","doi":"10.1186/s13037-024-00419-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The clinical benefit of locking plates in distal fibula fractures has not yet been proven. In addition, the risk of wound complications appears to be higher than with conventional tubular plates. We hypothesize that the benefits of locking plates in terms of biomechanical properties are outweighed by a higher risk of wound complications.</p><p><strong>Methods: </strong>We conducted a retrospective review of fibula fractures treated by osteosynthesis with either a conventional one-third tubular plate or an anatomically shaped locking plate from January 1, 2015 to December 31, 2021. We recorded baseline data and relevant comorbidities and defined the need for revision surgery due to wound-related or mechanical complications as primary endpoints.</p><p><strong>Results: </strong>A total of 595 out of 727 patients were eligible for our study. Of these 595 fractures, 526 were fixed with a one-third tubular plate, 69 with a locking plate. Revision surgery was required in 54 patients, in 51 cases due to wound complications. Three patients required revision surgery for mechanical reasons and all of them were younger than 40 years of age, have not been diagnosed with osteoporosis, but experienced complex fracture types. As the third tubular plate and locking plate groups differed in terms of age and comorbidities, we performed a 2:1 matching based on age and gender, leaving data from 138 patients receiving a third tubular plate. While the two groups were comparable in many aspects, the rate of wound complications was significantly higher in the locking plate group. Although the locking plate group had a higher percentage of diabetes mellitus, there was no correlation between this comorbidity and the higher revision rate in this group.</p><p><strong>Conclusions: </strong>Our data do not support the general use of locking plates in the treatment of distal fibular fractures. The risk of mechanical complications in osteoporotic ankle fractures seems to be overrated, as there were no mechanical revisions in the osteoporotic subgroup. The rate of wound-related revision surgery was significantly higher after the use of locking plates. This might be attributed to the greater thickness of locking plates.</p>","PeriodicalId":46782,"journal":{"name":"Patient Safety in Surgery","volume":"18 1","pages":"33"},"PeriodicalIF":2.1000,"publicationDate":"2024-12-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11613479/pdf/","citationCount":"0","resultStr":"{\"title\":\"Modern anatomical locking plates are associated with increased postoperative wound complications and unplanned surgical revisions compared to standard tubular plates in the management of unstable ankle fractures: a comparative cohort study in 595 patients.\",\"authors\":\"Patrick Gahr, Manuel Matthis, Lennart Schleese, Dagmar-C Fischer, Thomas Mittlmeier\",\"doi\":\"10.1186/s13037-024-00419-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The clinical benefit of locking plates in distal fibula fractures has not yet been proven. In addition, the risk of wound complications appears to be higher than with conventional tubular plates. We hypothesize that the benefits of locking plates in terms of biomechanical properties are outweighed by a higher risk of wound complications.</p><p><strong>Methods: </strong>We conducted a retrospective review of fibula fractures treated by osteosynthesis with either a conventional one-third tubular plate or an anatomically shaped locking plate from January 1, 2015 to December 31, 2021. We recorded baseline data and relevant comorbidities and defined the need for revision surgery due to wound-related or mechanical complications as primary endpoints.</p><p><strong>Results: </strong>A total of 595 out of 727 patients were eligible for our study. Of these 595 fractures, 526 were fixed with a one-third tubular plate, 69 with a locking plate. Revision surgery was required in 54 patients, in 51 cases due to wound complications. Three patients required revision surgery for mechanical reasons and all of them were younger than 40 years of age, have not been diagnosed with osteoporosis, but experienced complex fracture types. As the third tubular plate and locking plate groups differed in terms of age and comorbidities, we performed a 2:1 matching based on age and gender, leaving data from 138 patients receiving a third tubular plate. While the two groups were comparable in many aspects, the rate of wound complications was significantly higher in the locking plate group. Although the locking plate group had a higher percentage of diabetes mellitus, there was no correlation between this comorbidity and the higher revision rate in this group.</p><p><strong>Conclusions: </strong>Our data do not support the general use of locking plates in the treatment of distal fibular fractures. The risk of mechanical complications in osteoporotic ankle fractures seems to be overrated, as there were no mechanical revisions in the osteoporotic subgroup. The rate of wound-related revision surgery was significantly higher after the use of locking plates. This might be attributed to the greater thickness of locking plates.</p>\",\"PeriodicalId\":46782,\"journal\":{\"name\":\"Patient Safety in Surgery\",\"volume\":\"18 1\",\"pages\":\"33\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-12-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11613479/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Patient Safety in Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13037-024-00419-7\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Patient Safety in Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13037-024-00419-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
Modern anatomical locking plates are associated with increased postoperative wound complications and unplanned surgical revisions compared to standard tubular plates in the management of unstable ankle fractures: a comparative cohort study in 595 patients.
Background: The clinical benefit of locking plates in distal fibula fractures has not yet been proven. In addition, the risk of wound complications appears to be higher than with conventional tubular plates. We hypothesize that the benefits of locking plates in terms of biomechanical properties are outweighed by a higher risk of wound complications.
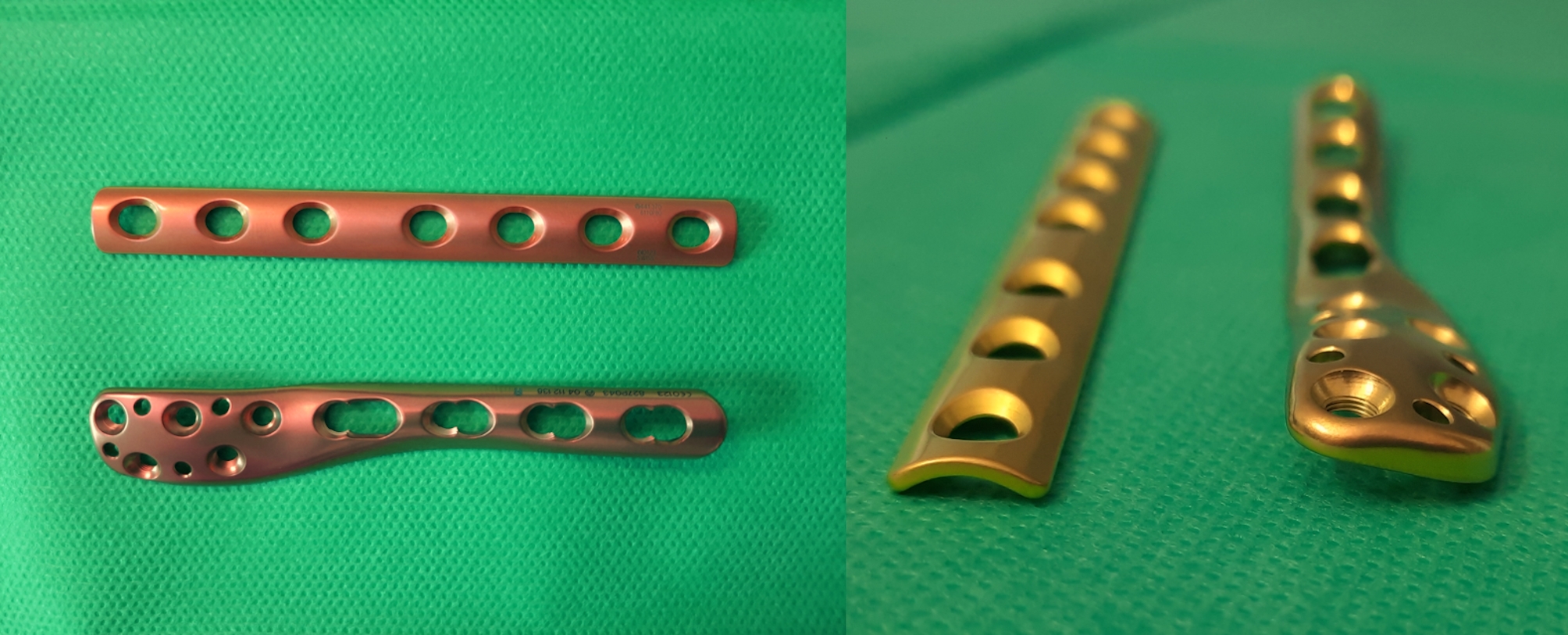
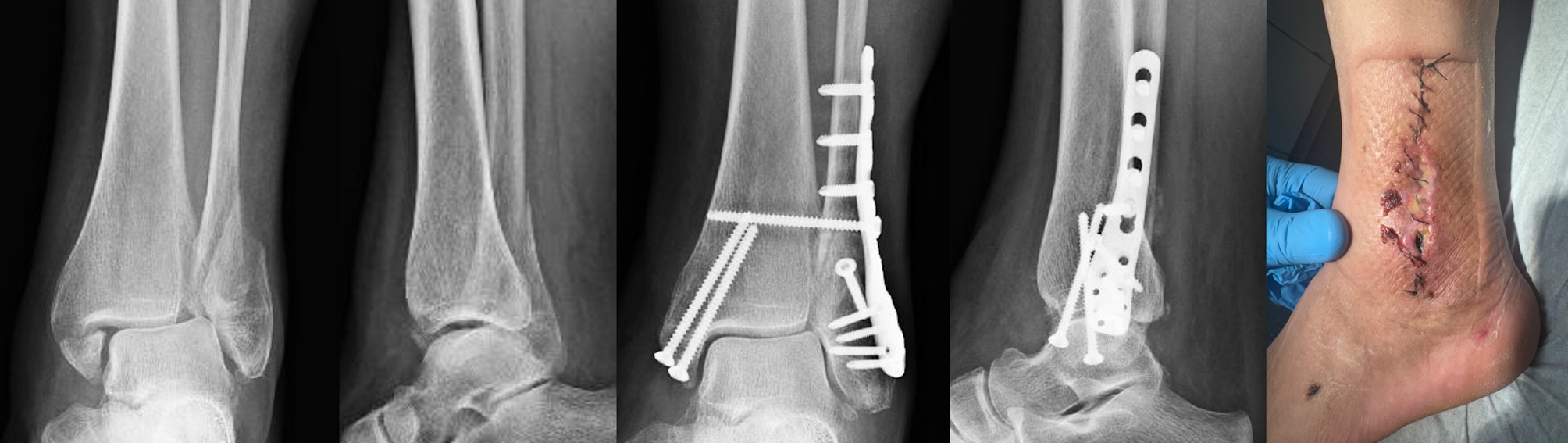
Methods: We conducted a retrospective review of fibula fractures treated by osteosynthesis with either a conventional one-third tubular plate or an anatomically shaped locking plate from January 1, 2015 to December 31, 2021. We recorded baseline data and relevant comorbidities and defined the need for revision surgery due to wound-related or mechanical complications as primary endpoints.
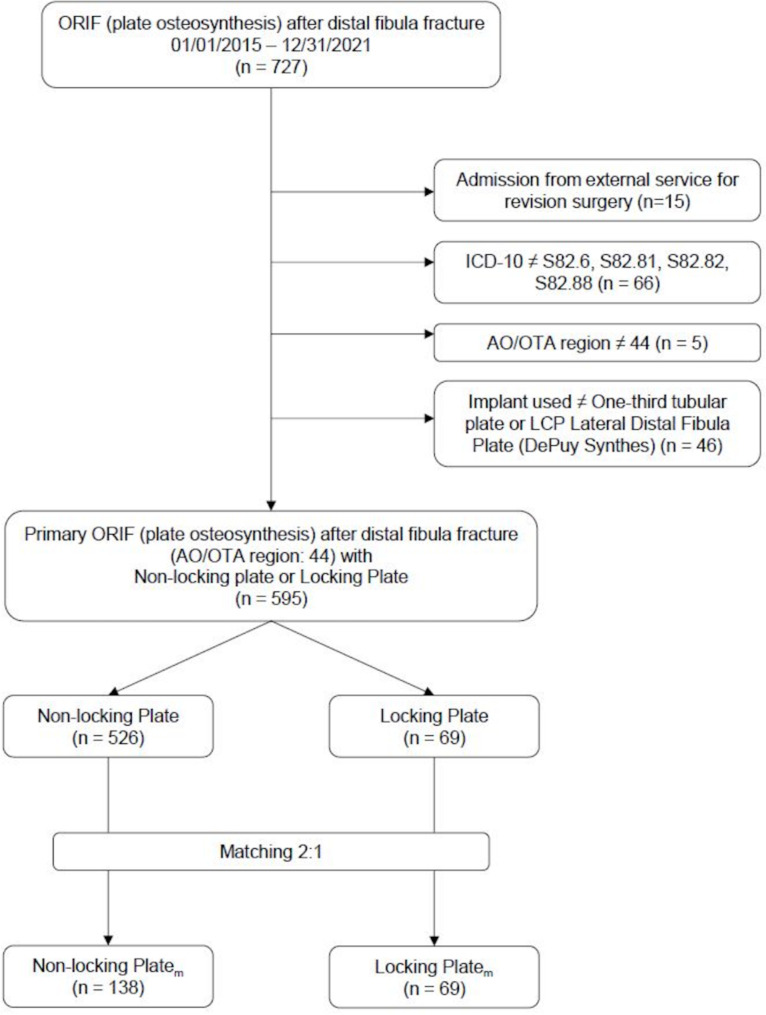
Results: A total of 595 out of 727 patients were eligible for our study. Of these 595 fractures, 526 were fixed with a one-third tubular plate, 69 with a locking plate. Revision surgery was required in 54 patients, in 51 cases due to wound complications. Three patients required revision surgery for mechanical reasons and all of them were younger than 40 years of age, have not been diagnosed with osteoporosis, but experienced complex fracture types. As the third tubular plate and locking plate groups differed in terms of age and comorbidities, we performed a 2:1 matching based on age and gender, leaving data from 138 patients receiving a third tubular plate. While the two groups were comparable in many aspects, the rate of wound complications was significantly higher in the locking plate group. Although the locking plate group had a higher percentage of diabetes mellitus, there was no correlation between this comorbidity and the higher revision rate in this group.
Conclusions: Our data do not support the general use of locking plates in the treatment of distal fibular fractures. The risk of mechanical complications in osteoporotic ankle fractures seems to be overrated, as there were no mechanical revisions in the osteoporotic subgroup. The rate of wound-related revision surgery was significantly higher after the use of locking plates. This might be attributed to the greater thickness of locking plates.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


