Sophia Gorgens, Ella R Rastegar, Manuel Beltran Del Rio, Cristy Meyer, Daniel M Rolston, Maria Sfakianos, Eric N Klein, Timmy Li, Rashmeet Gujral, Matthew A Bank, Daniel Jafari
{"title":"交通模式和紧急医疗服务在创伤激活中的预通知运输估计。","authors":"Sophia Gorgens, Ella R Rastegar, Manuel Beltran Del Rio, Cristy Meyer, Daniel M Rolston, Maria Sfakianos, Eric N Klein, Timmy Li, Rashmeet Gujral, Matthew A Bank, Daniel Jafari","doi":"10.2147/OAEM.S480081","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To determine whether traffic patterns affect the accuracy of emergency medical services (EMS) prediction of transport interval to the emergency department (ED).</p><p><strong>Methods: </strong>Using a retrospective study, we examined all trauma activations at a level one, urban trauma center in Manhasset, New York, between 5/22/2021 and 3/30/2022. Inclusion criteria included patients ≥18 years and arrival by EMS. Field trauma activations involve prenotification communication through a government intermediary. Transport during \"peak hours\" was defined as hospital arrival of EMS between 06:00-10:00 and 16:00-20:00, Monday through Friday. ETI and actual transit interval (ATI) were extracted from the recorded prenotification calls and hospital records respectively. In instances with a time range, the arithmetic mean was used. ATI was defined as the time from prenotification call to arrival at the hospital. A 25% difference between EMS ETI and ATI was chosen to categorize each arrival as overestimated (ATI/ETI < 0.75), accurate (ATI/ETI within 0.75-1.25), and underestimated (ATI/ETI > 1.25). Fisher's exact and Wilcoxon Rank Sum tests were used for comparative analysis as appropriate.</p><p><strong>Results: </strong>Of the 369 trauma transports, 117 had prenotification reports with an ETI and were included in our analysis. Of those, 29 (25%) occurred during peak hours. Overall, EMS more often underestimated ETI (55%) than exactly (32%), or overestimated ETI (12%) (p<0.0001). This was true during peak and off-peak hours with underestimated, accurate, and overestimated arrivals being 59%, 31%, 10% (p<0.01); and 54%, 33%, 12% (p<0.001), respectively. There was no statistically significant difference between peak vs off-peak hours when comparing the proportion of under vs over-estimated times of arrival (p=0.263).</p><p><strong>Conclusion: </strong>While our hypothesis was not borne out, further research on the antecedents of underestimated transport intervals in traumas is warranted. This will allow for targeted solutions to best support EMS clinicians in communicating transport times back to the ED.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"16 ","pages":"297-303"},"PeriodicalIF":1.5000,"publicationDate":"2024-11-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11613700/pdf/","citationCount":"0","resultStr":"{\"title\":\"Traffic Patterns and Emergency Medical Services Prenotification Transport Estimates in Trauma Activations.\",\"authors\":\"Sophia Gorgens, Ella R Rastegar, Manuel Beltran Del Rio, Cristy Meyer, Daniel M Rolston, Maria Sfakianos, Eric N Klein, Timmy Li, Rashmeet Gujral, Matthew A Bank, Daniel Jafari\",\"doi\":\"10.2147/OAEM.S480081\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To determine whether traffic patterns affect the accuracy of emergency medical services (EMS) prediction of transport interval to the emergency department (ED).</p><p><strong>Methods: </strong>Using a retrospective study, we examined all trauma activations at a level one, urban trauma center in Manhasset, New York, between 5/22/2021 and 3/30/2022. Inclusion criteria included patients ≥18 years and arrival by EMS. Field trauma activations involve prenotification communication through a government intermediary. Transport during \\\"peak hours\\\" was defined as hospital arrival of EMS between 06:00-10:00 and 16:00-20:00, Monday through Friday. ETI and actual transit interval (ATI) were extracted from the recorded prenotification calls and hospital records respectively. In instances with a time range, the arithmetic mean was used. ATI was defined as the time from prenotification call to arrival at the hospital. A 25% difference between EMS ETI and ATI was chosen to categorize each arrival as overestimated (ATI/ETI < 0.75), accurate (ATI/ETI within 0.75-1.25), and underestimated (ATI/ETI > 1.25). Fisher's exact and Wilcoxon Rank Sum tests were used for comparative analysis as appropriate.</p><p><strong>Results: </strong>Of the 369 trauma transports, 117 had prenotification reports with an ETI and were included in our analysis. Of those, 29 (25%) occurred during peak hours. Overall, EMS more often underestimated ETI (55%) than exactly (32%), or overestimated ETI (12%) (p<0.0001). This was true during peak and off-peak hours with underestimated, accurate, and overestimated arrivals being 59%, 31%, 10% (p<0.01); and 54%, 33%, 12% (p<0.001), respectively. There was no statistically significant difference between peak vs off-peak hours when comparing the proportion of under vs over-estimated times of arrival (p=0.263).</p><p><strong>Conclusion: </strong>While our hypothesis was not borne out, further research on the antecedents of underestimated transport intervals in traumas is warranted. This will allow for targeted solutions to best support EMS clinicians in communicating transport times back to the ED.</p>\",\"PeriodicalId\":45096,\"journal\":{\"name\":\"Open Access Emergency Medicine\",\"volume\":\"16 \",\"pages\":\"297-303\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2024-11-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11613700/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Access Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OAEM.S480081\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S480081","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Traffic Patterns and Emergency Medical Services Prenotification Transport Estimates in Trauma Activations.
Objective: To determine whether traffic patterns affect the accuracy of emergency medical services (EMS) prediction of transport interval to the emergency department (ED).
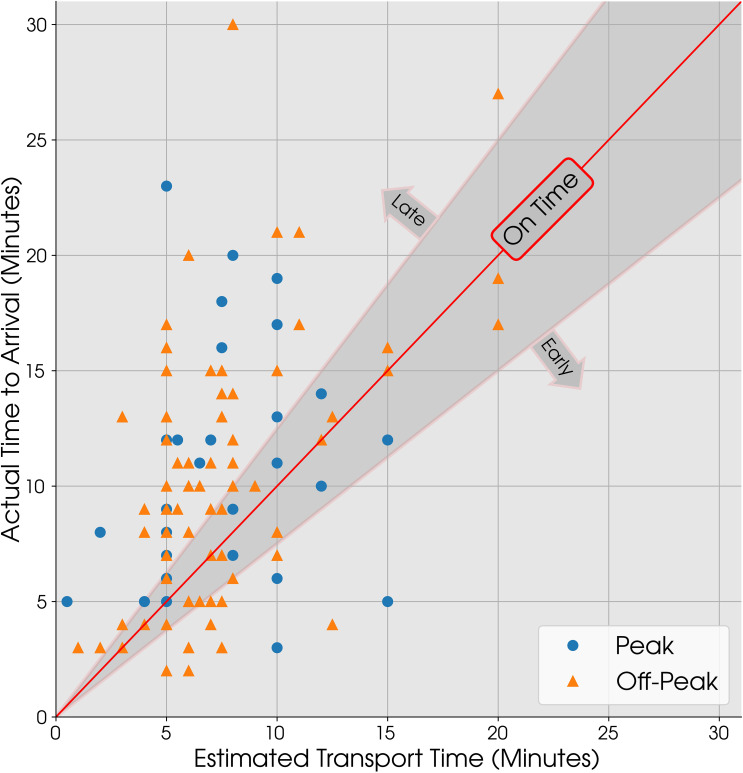
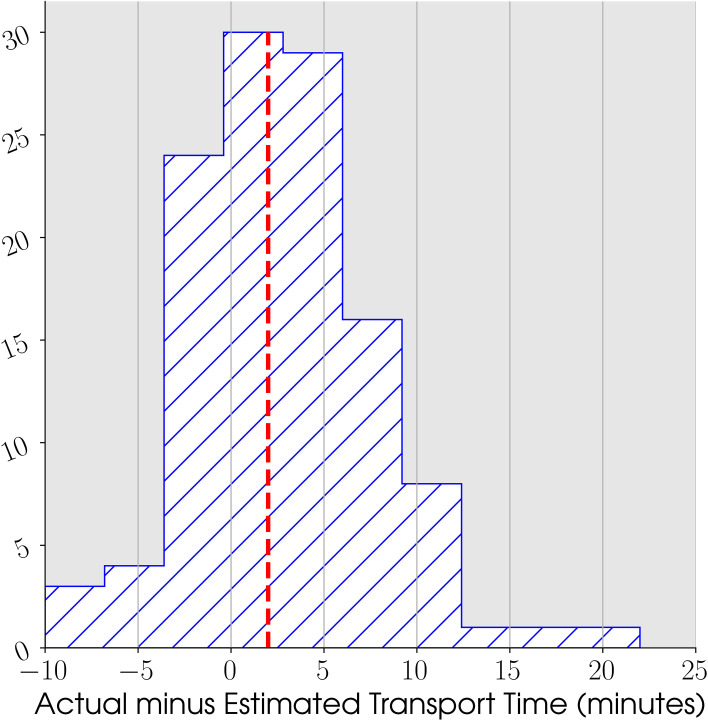
Methods: Using a retrospective study, we examined all trauma activations at a level one, urban trauma center in Manhasset, New York, between 5/22/2021 and 3/30/2022. Inclusion criteria included patients ≥18 years and arrival by EMS. Field trauma activations involve prenotification communication through a government intermediary. Transport during "peak hours" was defined as hospital arrival of EMS between 06:00-10:00 and 16:00-20:00, Monday through Friday. ETI and actual transit interval (ATI) were extracted from the recorded prenotification calls and hospital records respectively. In instances with a time range, the arithmetic mean was used. ATI was defined as the time from prenotification call to arrival at the hospital. A 25% difference between EMS ETI and ATI was chosen to categorize each arrival as overestimated (ATI/ETI < 0.75), accurate (ATI/ETI within 0.75-1.25), and underestimated (ATI/ETI > 1.25). Fisher's exact and Wilcoxon Rank Sum tests were used for comparative analysis as appropriate.
Results: Of the 369 trauma transports, 117 had prenotification reports with an ETI and were included in our analysis. Of those, 29 (25%) occurred during peak hours. Overall, EMS more often underestimated ETI (55%) than exactly (32%), or overestimated ETI (12%) (p<0.0001). This was true during peak and off-peak hours with underestimated, accurate, and overestimated arrivals being 59%, 31%, 10% (p<0.01); and 54%, 33%, 12% (p<0.001), respectively. There was no statistically significant difference between peak vs off-peak hours when comparing the proportion of under vs over-estimated times of arrival (p=0.263).
Conclusion: While our hypothesis was not borne out, further research on the antecedents of underestimated transport intervals in traumas is warranted. This will allow for targeted solutions to best support EMS clinicians in communicating transport times back to the ED.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


