{"title":"当自由空气不在隔膜下面时","authors":"Andrew K. Chiu, Zinta Zapp MD","doi":"10.1002/emp2.13275","DOIUrl":null,"url":null,"abstract":"<p>A 52-year-old woman presented to the emergency department with 3 days of abdominal pain. The pain began 1 day after undergoing a screening colonoscopy. On examination, her vital signs were normal and she had significant tenderness to the lower abdomen. Laboratory work revealed a white count of 22 K/µL and a normal lactate (0.8 mmol/L). An upright chest and abdominal x-ray were normal. Computed tomography (CT) of the abdomen with intravenous (IV) contrast was then performed.</p><p>Intestinal perforation is a potentially life-threatening complication that may arise from diverse etiologies, including instrumentation.<span><sup>1-4</sup></span> The initial step in workup of suspected intestinal perforation is often looking for free air under the diaphragm on an upright abdominal x-ray to evaluate for pneumoperitoneum.<span><sup>1</sup></span> We would not see this finding in our patient because she had pneumoretroperitoneum, where the gas pattern is different from that of pneumoperitoneum.<span><sup>5</sup></span> Ultimately, CT scan showed retroperitoneal air tracking along the aorta and inferior vena cava (IVC) (Figures 1 and 2). She underwent exploratory laparotomy with creation of a diverting end descending colostomy.</p><p>Colonoscopy-related perforation (CRP) is rare; the incidence ranges from 0.016% to 0.2% following diagnostic procedures and up to 5%, if the colonoscopy is therapeutic.<span><sup>2-4</sup></span> Rectal perforations, as in this case, have been reported to have an incidence ranging from 0.003% to 0.01%.<span><sup>2, 6</sup></span> CRP can be managed conservatively or surgically. It is important to note that up to 31% of patients with CRP present for treatment more than 24 h after their colonoscopy.<span><sup>3, 4</sup></span></p>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 6","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-11-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13275","citationCount":"0","resultStr":"{\"title\":\"When free air is not under the diaphragm\",\"authors\":\"Andrew K. Chiu, Zinta Zapp MD\",\"doi\":\"10.1002/emp2.13275\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 52-year-old woman presented to the emergency department with 3 days of abdominal pain. The pain began 1 day after undergoing a screening colonoscopy. On examination, her vital signs were normal and she had significant tenderness to the lower abdomen. Laboratory work revealed a white count of 22 K/µL and a normal lactate (0.8 mmol/L). An upright chest and abdominal x-ray were normal. Computed tomography (CT) of the abdomen with intravenous (IV) contrast was then performed.</p><p>Intestinal perforation is a potentially life-threatening complication that may arise from diverse etiologies, including instrumentation.<span><sup>1-4</sup></span> The initial step in workup of suspected intestinal perforation is often looking for free air under the diaphragm on an upright abdominal x-ray to evaluate for pneumoperitoneum.<span><sup>1</sup></span> We would not see this finding in our patient because she had pneumoretroperitoneum, where the gas pattern is different from that of pneumoperitoneum.<span><sup>5</sup></span> Ultimately, CT scan showed retroperitoneal air tracking along the aorta and inferior vena cava (IVC) (Figures 1 and 2). She underwent exploratory laparotomy with creation of a diverting end descending colostomy.</p><p>Colonoscopy-related perforation (CRP) is rare; the incidence ranges from 0.016% to 0.2% following diagnostic procedures and up to 5%, if the colonoscopy is therapeutic.<span><sup>2-4</sup></span> Rectal perforations, as in this case, have been reported to have an incidence ranging from 0.003% to 0.01%.<span><sup>2, 6</sup></span> CRP can be managed conservatively or surgically. It is important to note that up to 31% of patients with CRP present for treatment more than 24 h after their colonoscopy.<span><sup>3, 4</sup></span></p>\",\"PeriodicalId\":73967,\"journal\":{\"name\":\"Journal of the American College of Emergency Physicians open\",\"volume\":\"5 6\",\"pages\":\"\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-11-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13275\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American College of Emergency Physicians open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13275\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13275","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
A 52-year-old woman presented to the emergency department with 3 days of abdominal pain. The pain began 1 day after undergoing a screening colonoscopy. On examination, her vital signs were normal and she had significant tenderness to the lower abdomen. Laboratory work revealed a white count of 22 K/µL and a normal lactate (0.8 mmol/L). An upright chest and abdominal x-ray were normal. Computed tomography (CT) of the abdomen with intravenous (IV) contrast was then performed.
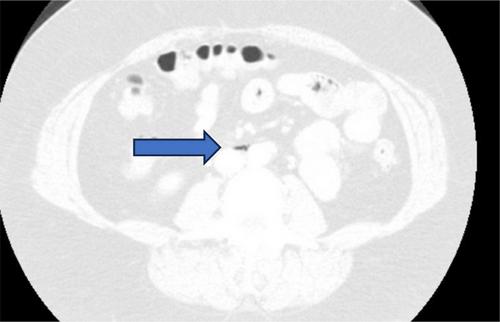
Intestinal perforation is a potentially life-threatening complication that may arise from diverse etiologies, including instrumentation.1-4 The initial step in workup of suspected intestinal perforation is often looking for free air under the diaphragm on an upright abdominal x-ray to evaluate for pneumoperitoneum.1 We would not see this finding in our patient because she had pneumoretroperitoneum, where the gas pattern is different from that of pneumoperitoneum.5 Ultimately, CT scan showed retroperitoneal air tracking along the aorta and inferior vena cava (IVC) (Figures 1 and 2). She underwent exploratory laparotomy with creation of a diverting end descending colostomy.
Colonoscopy-related perforation (CRP) is rare; the incidence ranges from 0.016% to 0.2% following diagnostic procedures and up to 5%, if the colonoscopy is therapeutic.2-4 Rectal perforations, as in this case, have been reported to have an incidence ranging from 0.003% to 0.01%.2, 6 CRP can be managed conservatively or surgically. It is important to note that up to 31% of patients with CRP present for treatment more than 24 h after their colonoscopy.3, 4

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


