Sergi Codina, Laia Oliveras, Eva Ferreiro, Aroa Rovira, Ana Coloma, Nuria Lloberas, Edoardo Melilli, Miguel Hueso, Fabrizio Sbraga, Enric Boza, José M Vazquez, José L Pérez-Fernández, Joan Sabater, Josep M Cruzado, Nuria Montero
{"title":"为避免心脏手术候诊患者急性肾损伤而进行的肾脏病干预:随机临床试验。","authors":"Sergi Codina, Laia Oliveras, Eva Ferreiro, Aroa Rovira, Ana Coloma, Nuria Lloberas, Edoardo Melilli, Miguel Hueso, Fabrizio Sbraga, Enric Boza, José M Vazquez, José L Pérez-Fernández, Joan Sabater, Josep M Cruzado, Nuria Montero","doi":"10.3389/fneph.2024.1470926","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Cardiac surgery-associated acute kidney injury (CSA-AKI) is a well-known complication that increases morbidity and mortality rates. The objective of this study was to reduce CSA-AKI through nephrologist intervention in patients awaiting cardiac surgery.</p><p><strong>Methods: </strong>We performed a single center, open-label, randomized clinical trial including 380 patients who underwent scheduled cardiac surgery at the Hospital de Bellvitge between July 2015 and October 2019. A total of 184 patients were evaluated by the same Nephrologist one month before the surgery to minimize the risk factors for AKI. In addition to assessments at the outpatient clinic, we also collected clinical data during hospitalization and during the first year.</p><p><strong>Results: </strong>Despite the intervention, no differences were observed between the groups in the incidence of CSA-AKI (intervention group 26.37% vs. standard of care 25.13%, p=0.874), mortality (3.91% vs. 3.59%, p=0.999), length of Intensive Care Unit (ICU) stay (10 days [7.00;15.0] for both groups, p=0.347), or renal function after one year of follow-up (estimated glomerular filtration rate (eGFR) by CKD-EPI: 74.5 ml/min (standard deviation 20.6) vs 76.7 (20.8) ml/min, respectively, p=0.364). A reduction in the need for blood transfusion was observed in the intervention group, although the difference was not statistically significant (37.22% vs. 45.03%, p =0.155).</p><p><strong>Conclusion: </strong>In this clinical trial, nephrologist intervention in the entire population on the cardiac surgery waiting list did not show a nephroprotective benefit.</p><p><strong>Clinical trial registration: </strong>ClinicalTrials.gov, identifier (NCT02643745).</p>","PeriodicalId":73091,"journal":{"name":"Frontiers in nephrology","volume":"4 ","pages":"1470926"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11599165/pdf/","citationCount":"0","resultStr":"{\"title\":\"Nephrology intervention to avoid acute kidney injury in patients awaiting cardiac surgery: randomized clinical trial.\",\"authors\":\"Sergi Codina, Laia Oliveras, Eva Ferreiro, Aroa Rovira, Ana Coloma, Nuria Lloberas, Edoardo Melilli, Miguel Hueso, Fabrizio Sbraga, Enric Boza, José M Vazquez, José L Pérez-Fernández, Joan Sabater, Josep M Cruzado, Nuria Montero\",\"doi\":\"10.3389/fneph.2024.1470926\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Cardiac surgery-associated acute kidney injury (CSA-AKI) is a well-known complication that increases morbidity and mortality rates. The objective of this study was to reduce CSA-AKI through nephrologist intervention in patients awaiting cardiac surgery.</p><p><strong>Methods: </strong>We performed a single center, open-label, randomized clinical trial including 380 patients who underwent scheduled cardiac surgery at the Hospital de Bellvitge between July 2015 and October 2019. A total of 184 patients were evaluated by the same Nephrologist one month before the surgery to minimize the risk factors for AKI. In addition to assessments at the outpatient clinic, we also collected clinical data during hospitalization and during the first year.</p><p><strong>Results: </strong>Despite the intervention, no differences were observed between the groups in the incidence of CSA-AKI (intervention group 26.37% vs. standard of care 25.13%, p=0.874), mortality (3.91% vs. 3.59%, p=0.999), length of Intensive Care Unit (ICU) stay (10 days [7.00;15.0] for both groups, p=0.347), or renal function after one year of follow-up (estimated glomerular filtration rate (eGFR) by CKD-EPI: 74.5 ml/min (standard deviation 20.6) vs 76.7 (20.8) ml/min, respectively, p=0.364). A reduction in the need for blood transfusion was observed in the intervention group, although the difference was not statistically significant (37.22% vs. 45.03%, p =0.155).</p><p><strong>Conclusion: </strong>In this clinical trial, nephrologist intervention in the entire population on the cardiac surgery waiting list did not show a nephroprotective benefit.</p><p><strong>Clinical trial registration: </strong>ClinicalTrials.gov, identifier (NCT02643745).</p>\",\"PeriodicalId\":73091,\"journal\":{\"name\":\"Frontiers in nephrology\",\"volume\":\"4 \",\"pages\":\"1470926\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-11-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11599165/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in nephrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/fneph.2024.1470926\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fneph.2024.1470926","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
导言:心脏手术相关急性肾损伤(CSA-AKI)是一种众所周知的并发症,会增加发病率和死亡率。本研究的目的是通过肾科医生对等待心脏手术的患者进行干预,减少 CSA-AKI 的发生:我们进行了一项单中心、开放标签、随机临床试验,包括 2015 年 7 月至 2019 年 10 月期间在贝尔维日医院接受预定心脏手术的 380 名患者。共有 184 名患者在手术前一个月接受了同一位肾脏科医生的评估,以尽量减少 AKI 的风险因素。除了在门诊进行评估外,我们还收集了住院期间和第一年的临床数据:尽管采取了干预措施,但两组在 CSA-AKI 发生率(干预组 26.37% vs. 标准护理组 25.13%,P=0.874)、死亡率(3.91% vs. 3.59%,P=0.999)、重症监护室(ICU)住院时间(两组均为 10 天 [7.P=0.347),或随访一年后的肾功能(根据 CKD-EPI 估计的肾小球滤过率(eGFR):分别为 74.5 毫升/分钟(标准差 20.6) vs 76.7 (20.8) 毫升/分钟,P=0.364)。干预组的输血需求有所减少,但差异无统计学意义(37.22% 对 45.03%,P=0.155):结论:在这项临床试验中,肾科医生对所有心脏手术候诊者的干预并未显示出保护肾脏的益处:临床试验注册:ClinicalTrials.gov,标识符(NCT02643745)。
Nephrology intervention to avoid acute kidney injury in patients awaiting cardiac surgery: randomized clinical trial.
Introduction: Cardiac surgery-associated acute kidney injury (CSA-AKI) is a well-known complication that increases morbidity and mortality rates. The objective of this study was to reduce CSA-AKI through nephrologist intervention in patients awaiting cardiac surgery.
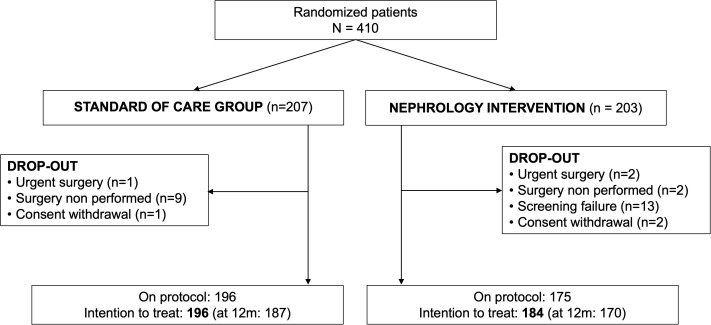
Methods: We performed a single center, open-label, randomized clinical trial including 380 patients who underwent scheduled cardiac surgery at the Hospital de Bellvitge between July 2015 and October 2019. A total of 184 patients were evaluated by the same Nephrologist one month before the surgery to minimize the risk factors for AKI. In addition to assessments at the outpatient clinic, we also collected clinical data during hospitalization and during the first year.
Results: Despite the intervention, no differences were observed between the groups in the incidence of CSA-AKI (intervention group 26.37% vs. standard of care 25.13%, p=0.874), mortality (3.91% vs. 3.59%, p=0.999), length of Intensive Care Unit (ICU) stay (10 days [7.00;15.0] for both groups, p=0.347), or renal function after one year of follow-up (estimated glomerular filtration rate (eGFR) by CKD-EPI: 74.5 ml/min (standard deviation 20.6) vs 76.7 (20.8) ml/min, respectively, p=0.364). A reduction in the need for blood transfusion was observed in the intervention group, although the difference was not statistically significant (37.22% vs. 45.03%, p =0.155).
Conclusion: In this clinical trial, nephrologist intervention in the entire population on the cardiac surgery waiting list did not show a nephroprotective benefit.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


