{"title":"动脉期 CT 在鉴别良好/不良冲洗肾上腺肿块中的嗜铬细胞瘤方面具有很高的诊断准确性。","authors":"Aditya Phadte, Brijesh Krishnappa, Saba Samad Memon, Virendra Patil, Anurag Lila, Padma Vikram Badhe, Vijaya Sarathi, Gwendolyn Fernandes, Sameer Rege, Gagan Prakash, Santosh Menon, Manjiri Karlekar, Rohit Barnabas, Nalini Shah, Hemangini Thakkar, Tushar Bandgar","doi":"10.1210/jendso/bvae199","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Differentiating pheochromocytomas from other adrenal masses based on computed tomography (CT) characteristics remains challenging, particularly in lipid-poor lesions with variable washout patterns. This study evaluated CT features for distinguishing pheochromocytomas in good and poor washout subcohorts.</p><p><strong>Methods: </strong>We prospectively analyzed 72 patients with unilateral lipid-poor adrenal masses. CT protocol included basal, bolus-tracked arterial, early venous (45 seconds postarterial), and delayed (15 minutes postarterial) phases. Masses were categorized into good and poor washout groups. Histopathology provided the final diagnosis. CT characteristics and calculated indices were compared between pheochromocytomas and other masses in each washout category.</p><p><strong>Results: </strong>The cohort included pheochromocytomas (n = 35), adrenocortical carcinoma (ACC; n = 15), lipid-poor adenomas (n = 13), and metastatic infiltration/infection (n = 9). In the good washout group, pheochromocytomas (n = 15) showed larger diameters (6.00 vs 3.45 cm, <i>P</i> = .001), higher necrosis frequency (73.3% vs 30%, <i>P</i> = .049), and greater arterial attenuation (173.2 vs 74.5 HU, <i>P</i> < .001) compared to adenomas (n = 9). Arterial attenuation provided a high discriminatory value [area under the curve (AUC): 0.967], with 100% sensitivity at 87.6 Hounsfield unit (HU) and 100% specificity at 139.9 HU. In the poor washout group, pheochromocytomas (n = 20) exhibited higher arterial attenuation (99.2 vs 59.2 HU, <i>P</i> < .001; AUC: 0.844) compared to ACC (n = 14), metastatic infiltration (n = 9), and adenomas (n = 4), with 85% sensitivity and 78% specificity at 73.3 HU. Normetanephrine-secreting/nonsecretory pheochromocytomas showed higher arterial enhancement than metanephrine-secreting ones (132.0 vs 90.5 HU, <i>P</i> = .020) within the poor washout group.</p><p><strong>Conclusion: </strong>Arterial phase attenuation on CT has good diagnostic accuracy for differentiating pheochromocytomas from other adrenal masses in both good and poor washout categories, potentially guiding hormonal workup.</p>","PeriodicalId":17334,"journal":{"name":"Journal of the Endocrine Society","volume":"9 1","pages":"bvae199"},"PeriodicalIF":3.1000,"publicationDate":"2024-11-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11590661/pdf/","citationCount":"0","resultStr":"{\"title\":\"High Diagnostic Accuracy of Arterial Phase CT in Differentiating Pheochromocytoma in Good/Poor Washout Adrenal Masses.\",\"authors\":\"Aditya Phadte, Brijesh Krishnappa, Saba Samad Memon, Virendra Patil, Anurag Lila, Padma Vikram Badhe, Vijaya Sarathi, Gwendolyn Fernandes, Sameer Rege, Gagan Prakash, Santosh Menon, Manjiri Karlekar, Rohit Barnabas, Nalini Shah, Hemangini Thakkar, Tushar Bandgar\",\"doi\":\"10.1210/jendso/bvae199\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Differentiating pheochromocytomas from other adrenal masses based on computed tomography (CT) characteristics remains challenging, particularly in lipid-poor lesions with variable washout patterns. This study evaluated CT features for distinguishing pheochromocytomas in good and poor washout subcohorts.</p><p><strong>Methods: </strong>We prospectively analyzed 72 patients with unilateral lipid-poor adrenal masses. CT protocol included basal, bolus-tracked arterial, early venous (45 seconds postarterial), and delayed (15 minutes postarterial) phases. Masses were categorized into good and poor washout groups. Histopathology provided the final diagnosis. CT characteristics and calculated indices were compared between pheochromocytomas and other masses in each washout category.</p><p><strong>Results: </strong>The cohort included pheochromocytomas (n = 35), adrenocortical carcinoma (ACC; n = 15), lipid-poor adenomas (n = 13), and metastatic infiltration/infection (n = 9). In the good washout group, pheochromocytomas (n = 15) showed larger diameters (6.00 vs 3.45 cm, <i>P</i> = .001), higher necrosis frequency (73.3% vs 30%, <i>P</i> = .049), and greater arterial attenuation (173.2 vs 74.5 HU, <i>P</i> < .001) compared to adenomas (n = 9). Arterial attenuation provided a high discriminatory value [area under the curve (AUC): 0.967], with 100% sensitivity at 87.6 Hounsfield unit (HU) and 100% specificity at 139.9 HU. In the poor washout group, pheochromocytomas (n = 20) exhibited higher arterial attenuation (99.2 vs 59.2 HU, <i>P</i> < .001; AUC: 0.844) compared to ACC (n = 14), metastatic infiltration (n = 9), and adenomas (n = 4), with 85% sensitivity and 78% specificity at 73.3 HU. Normetanephrine-secreting/nonsecretory pheochromocytomas showed higher arterial enhancement than metanephrine-secreting ones (132.0 vs 90.5 HU, <i>P</i> = .020) within the poor washout group.</p><p><strong>Conclusion: </strong>Arterial phase attenuation on CT has good diagnostic accuracy for differentiating pheochromocytomas from other adrenal masses in both good and poor washout categories, potentially guiding hormonal workup.</p>\",\"PeriodicalId\":17334,\"journal\":{\"name\":\"Journal of the Endocrine Society\",\"volume\":\"9 1\",\"pages\":\"bvae199\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2024-11-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11590661/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Endocrine Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1210/jendso/bvae199\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/26 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Endocrine Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jendso/bvae199","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/26 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
摘要
导言:根据计算机断层扫描(CT)特征区分嗜铬细胞瘤和其他肾上腺肿块仍具有挑战性,尤其是在冲洗模式多变的贫脂病变中。本研究评估了在冲洗良好和冲洗不良亚群中区分嗜铬细胞瘤的 CT 特征:我们对 72 例单侧贫脂肾上腺肿块患者进行了前瞻性分析。CT方案包括基础期、栓剂追踪动脉期、早期静脉期(动脉后45秒)和延迟期(动脉后15分钟)。肿块被分为冲洗良好组和冲洗不良组。组织病理学提供最终诊断。对每个冲洗组中嗜铬细胞瘤和其他肿块的 CT 特征和计算指数进行比较:结果:队列包括嗜铬细胞瘤(35 例)、肾上腺皮质癌(15 例)、贫脂腺瘤(13 例)和转移性浸润/感染(9 例)。在良好冲洗组中,与腺瘤(n = 9)相比,嗜铬细胞瘤(n = 15)直径更大(6.00 vs 3.45 cm,P = .001),坏死频率更高(73.3% vs 30%,P = .049),动脉衰减更大(173.2 vs 74.5 HU,P < .001)。动脉衰减具有很高的鉴别价值[曲线下面积(AUC):0.967],87.6 Hounsfield 单位(HU)的灵敏度为 100%,139.9 HU 的特异性为 100%。在冲洗不良组中,嗜铬细胞瘤(n = 20)与 ACC(n = 14)、转移性浸润(n = 9)和腺瘤(n = 4)相比,动脉衰减更高(99.2 vs 59.2 HU,P < .001;AUC:0.844),在 73.3 HU 时灵敏度为 85%,特异性为 78%。在冲洗不良组中,正常分泌肾上腺素/非分泌型嗜铬细胞瘤的动脉强化高于分泌肾上腺素的嗜铬细胞瘤(132.0 HU vs 90.5 HU,P = .020):结论:CT上的动脉相位衰减对鉴别嗜铬细胞瘤和其他肾上腺肿块具有良好的诊断准确性,无论是冲洗良好组还是冲洗不良组,都有可能为激素治疗提供指导。
High Diagnostic Accuracy of Arterial Phase CT in Differentiating Pheochromocytoma in Good/Poor Washout Adrenal Masses.
Introduction: Differentiating pheochromocytomas from other adrenal masses based on computed tomography (CT) characteristics remains challenging, particularly in lipid-poor lesions with variable washout patterns. This study evaluated CT features for distinguishing pheochromocytomas in good and poor washout subcohorts.
Methods: We prospectively analyzed 72 patients with unilateral lipid-poor adrenal masses. CT protocol included basal, bolus-tracked arterial, early venous (45 seconds postarterial), and delayed (15 minutes postarterial) phases. Masses were categorized into good and poor washout groups. Histopathology provided the final diagnosis. CT characteristics and calculated indices were compared between pheochromocytomas and other masses in each washout category.
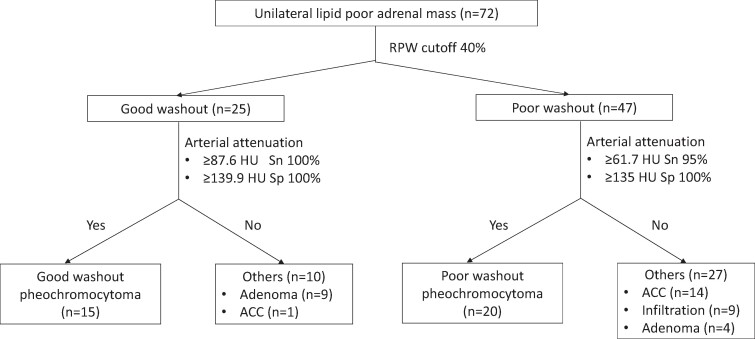
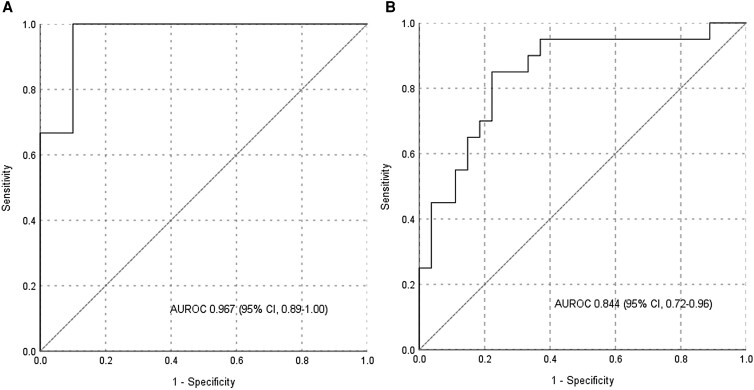
Results: The cohort included pheochromocytomas (n = 35), adrenocortical carcinoma (ACC; n = 15), lipid-poor adenomas (n = 13), and metastatic infiltration/infection (n = 9). In the good washout group, pheochromocytomas (n = 15) showed larger diameters (6.00 vs 3.45 cm, P = .001), higher necrosis frequency (73.3% vs 30%, P = .049), and greater arterial attenuation (173.2 vs 74.5 HU, P < .001) compared to adenomas (n = 9). Arterial attenuation provided a high discriminatory value [area under the curve (AUC): 0.967], with 100% sensitivity at 87.6 Hounsfield unit (HU) and 100% specificity at 139.9 HU. In the poor washout group, pheochromocytomas (n = 20) exhibited higher arterial attenuation (99.2 vs 59.2 HU, P < .001; AUC: 0.844) compared to ACC (n = 14), metastatic infiltration (n = 9), and adenomas (n = 4), with 85% sensitivity and 78% specificity at 73.3 HU. Normetanephrine-secreting/nonsecretory pheochromocytomas showed higher arterial enhancement than metanephrine-secreting ones (132.0 vs 90.5 HU, P = .020) within the poor washout group.
Conclusion: Arterial phase attenuation on CT has good diagnostic accuracy for differentiating pheochromocytomas from other adrenal masses in both good and poor washout categories, potentially guiding hormonal workup.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


