Laura A Magee, Katie Kirkham, Sue Tohill, Eleni Gkini, Catherine A Moakes, Jon Dorling, Marcus Green, Jennifer A Hutcheon, Mishal Javed, Jesse Kigozi, Ben W M Mol, Joel Singer, Pollyanna Hardy, Clive Stubbs, James G Thornton, Peter von Dadelszen
{"title":"确定患有慢性高血压或妊娠高血压的足月妇女的最佳分娩时间:WILL(何时引产以限制妊娠高血压风险)随机试验。","authors":"Laura A Magee, Katie Kirkham, Sue Tohill, Eleni Gkini, Catherine A Moakes, Jon Dorling, Marcus Green, Jennifer A Hutcheon, Mishal Javed, Jesse Kigozi, Ben W M Mol, Joel Singer, Pollyanna Hardy, Clive Stubbs, James G Thornton, Peter von Dadelszen","doi":"10.1371/journal.pmed.1004481","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic or gestational hypertension complicates approximately 7% of pregnancies, half of which reach 37 weeks' gestation. Early term birth (at 37 to 38 weeks) may reduce maternal complications, cesareans, stillbirths, and costs but may increase neonatal morbidity. In the WILL Trial (When to Induce Labour to Limit risk in pregnancy hypertension), we aimed to establish optimal timing of birth for women with chronic or gestational hypertension who reach term and remain well.</p><p><strong>Methods and findings: </strong>This 50-centre, open-label, randomised trial in the United Kingdom included an economic analysis. WILL randomised women with chronic or gestational hypertension at 36 to 37 weeks and a singleton fetus, and who provided documented informed consent to \"Planned early term birth at 38+0-3 weeks\" (intervention) or \"usual care at term\" (control). The coprimary outcomes were \"poor maternal outcome\" (composite of severe hypertension, maternal death, or maternal morbidity; superiority hypothesis) and \"neonatal care unit admission for ≥4 hours\" (noninferiority hypothesis). The key secondary was cesarean. Follow-up was to 6 weeks postpartum. The planned sample size was 540/group. Analysis was by intention-to-treat. A total of 403 participants (37.3% of target) were randomised to the intervention (n = 201) or control group (n = 202), from 3 June 2019 to 19 December 2022, when the funder stopped the trial for delayed recruitment. In the intervention (versus control) group, losses to follow-up were 18/201 (9%) versus 15/202 (7%). In each group, maternal age was about 30 years, about one-fifth of women were from ethnic minorities, over half had obesity, approximately half had chronic hypertension, and most were on antihypertensives with normal blood pressure. In the intervention (versus control) group, birth was a median of 0.9 weeks earlier (38.4 [38.3 to 38.6] versus 39.3 [38.7 to 39.9] weeks). There was no evidence of a difference in \"poor maternal outcome\" (27/201 [13%] versus 24/202 [12%], respectively; adjusted risk ratio [aRR] 1.16, 95% confidence interval [CI] 0.72 to 1.87). For \"neonatal care unit admission for ≥4 hours,\" the intervention was considered noninferior to the control as the adjusted risk difference (aRD) 95% CI upper bound did not cross the 8% prespecified noninferiority margin (14/201 [7%] versus 14/202 [7%], respectively; aRD 0.003, 95% CI -0.05 to +0.06), although event rates were lower-than-estimated. The intervention (versus control) was associated with no difference in cesarean (58/201 [29%] versus 72/202 [36%], respectively; aRR 0.81, 95% CI 0.61 to 1.08. There were no serious adverse events. Limitations include our smaller-than-planned sample size, and lower-than-anticipated event rates, so the findings may not be generalisable to where hypertension is not treated with antihypertensive therapy.</p><p><strong>Conclusions: </strong>In this study, we observed that most women with chronic or gestational hypertension required labour induction, and planned birth at 38+0-3 weeks (versus usual care) resulted in birth an average of 6 days earlier, and no differences in poor maternal outcome or neonatal morbidity. Our findings provide reassurance about planned birth at 38+0-3 weeks as a clinical option for these women.</p><p><strong>Trial registration: </strong>isrctn.com ISRCTN77258279.</p>","PeriodicalId":49008,"journal":{"name":"PLoS Medicine","volume":"21 11","pages":"e1004481"},"PeriodicalIF":9.9000,"publicationDate":"2024-11-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11593758/pdf/","citationCount":"0","resultStr":"{\"title\":\"Determining optimal timing of birth for women with chronic or gestational hypertension at term: The WILL (When to Induce Labour to Limit risk in pregnancy hypertension) randomised trial.\",\"authors\":\"Laura A Magee, Katie Kirkham, Sue Tohill, Eleni Gkini, Catherine A Moakes, Jon Dorling, Marcus Green, Jennifer A Hutcheon, Mishal Javed, Jesse Kigozi, Ben W M Mol, Joel Singer, Pollyanna Hardy, Clive Stubbs, James G Thornton, Peter von Dadelszen\",\"doi\":\"10.1371/journal.pmed.1004481\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Chronic or gestational hypertension complicates approximately 7% of pregnancies, half of which reach 37 weeks' gestation. Early term birth (at 37 to 38 weeks) may reduce maternal complications, cesareans, stillbirths, and costs but may increase neonatal morbidity. In the WILL Trial (When to Induce Labour to Limit risk in pregnancy hypertension), we aimed to establish optimal timing of birth for women with chronic or gestational hypertension who reach term and remain well.</p><p><strong>Methods and findings: </strong>This 50-centre, open-label, randomised trial in the United Kingdom included an economic analysis. WILL randomised women with chronic or gestational hypertension at 36 to 37 weeks and a singleton fetus, and who provided documented informed consent to \\\"Planned early term birth at 38+0-3 weeks\\\" (intervention) or \\\"usual care at term\\\" (control). The coprimary outcomes were \\\"poor maternal outcome\\\" (composite of severe hypertension, maternal death, or maternal morbidity; superiority hypothesis) and \\\"neonatal care unit admission for ≥4 hours\\\" (noninferiority hypothesis). The key secondary was cesarean. Follow-up was to 6 weeks postpartum. The planned sample size was 540/group. Analysis was by intention-to-treat. A total of 403 participants (37.3% of target) were randomised to the intervention (n = 201) or control group (n = 202), from 3 June 2019 to 19 December 2022, when the funder stopped the trial for delayed recruitment. In the intervention (versus control) group, losses to follow-up were 18/201 (9%) versus 15/202 (7%). In each group, maternal age was about 30 years, about one-fifth of women were from ethnic minorities, over half had obesity, approximately half had chronic hypertension, and most were on antihypertensives with normal blood pressure. In the intervention (versus control) group, birth was a median of 0.9 weeks earlier (38.4 [38.3 to 38.6] versus 39.3 [38.7 to 39.9] weeks). There was no evidence of a difference in \\\"poor maternal outcome\\\" (27/201 [13%] versus 24/202 [12%], respectively; adjusted risk ratio [aRR] 1.16, 95% confidence interval [CI] 0.72 to 1.87). For \\\"neonatal care unit admission for ≥4 hours,\\\" the intervention was considered noninferior to the control as the adjusted risk difference (aRD) 95% CI upper bound did not cross the 8% prespecified noninferiority margin (14/201 [7%] versus 14/202 [7%], respectively; aRD 0.003, 95% CI -0.05 to +0.06), although event rates were lower-than-estimated. The intervention (versus control) was associated with no difference in cesarean (58/201 [29%] versus 72/202 [36%], respectively; aRR 0.81, 95% CI 0.61 to 1.08. There were no serious adverse events. Limitations include our smaller-than-planned sample size, and lower-than-anticipated event rates, so the findings may not be generalisable to where hypertension is not treated with antihypertensive therapy.</p><p><strong>Conclusions: </strong>In this study, we observed that most women with chronic or gestational hypertension required labour induction, and planned birth at 38+0-3 weeks (versus usual care) resulted in birth an average of 6 days earlier, and no differences in poor maternal outcome or neonatal morbidity. Our findings provide reassurance about planned birth at 38+0-3 weeks as a clinical option for these women.</p><p><strong>Trial registration: </strong>isrctn.com ISRCTN77258279.</p>\",\"PeriodicalId\":49008,\"journal\":{\"name\":\"PLoS Medicine\",\"volume\":\"21 11\",\"pages\":\"e1004481\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2024-11-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11593758/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pmed.1004481\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1004481","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Determining optimal timing of birth for women with chronic or gestational hypertension at term: The WILL (When to Induce Labour to Limit risk in pregnancy hypertension) randomised trial.
Background: Chronic or gestational hypertension complicates approximately 7% of pregnancies, half of which reach 37 weeks' gestation. Early term birth (at 37 to 38 weeks) may reduce maternal complications, cesareans, stillbirths, and costs but may increase neonatal morbidity. In the WILL Trial (When to Induce Labour to Limit risk in pregnancy hypertension), we aimed to establish optimal timing of birth for women with chronic or gestational hypertension who reach term and remain well.
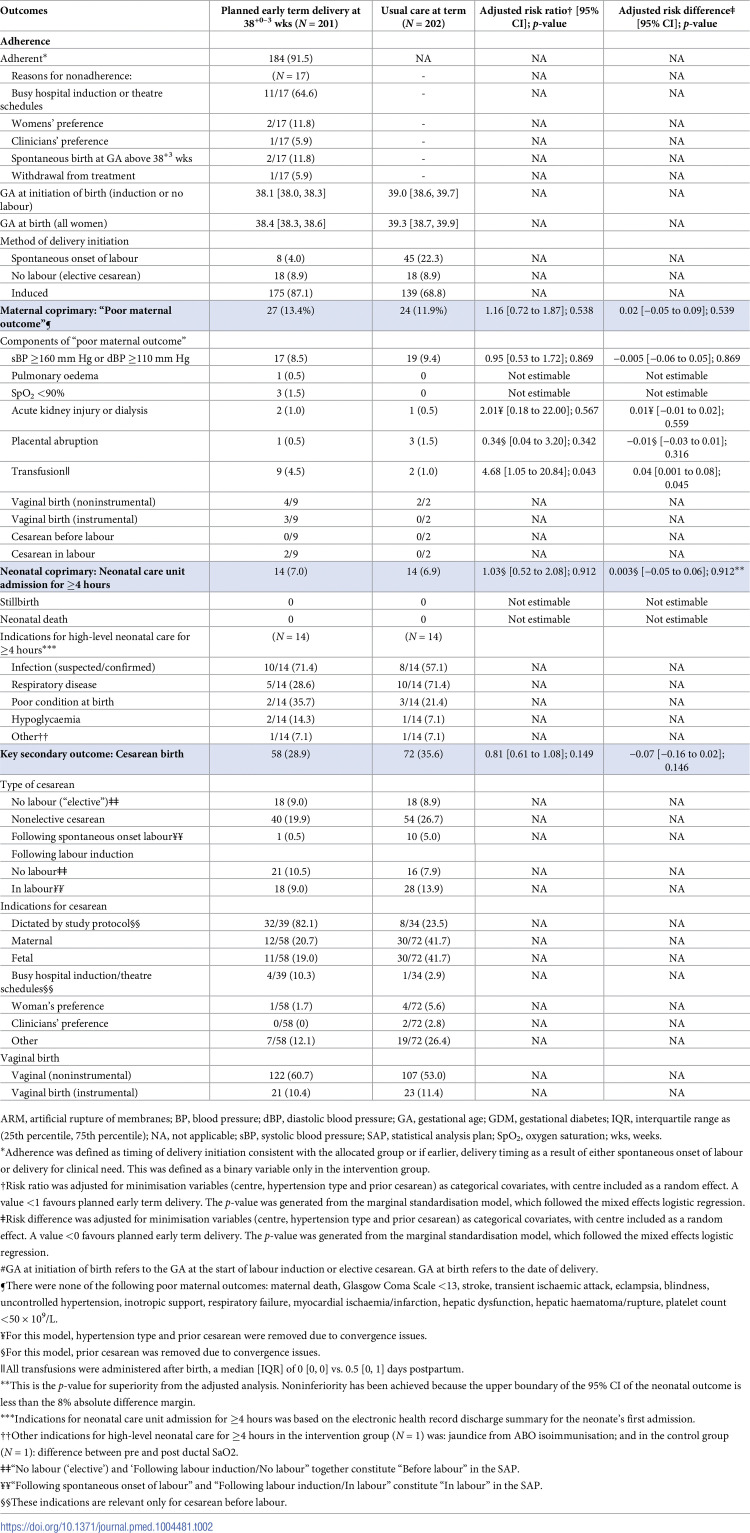
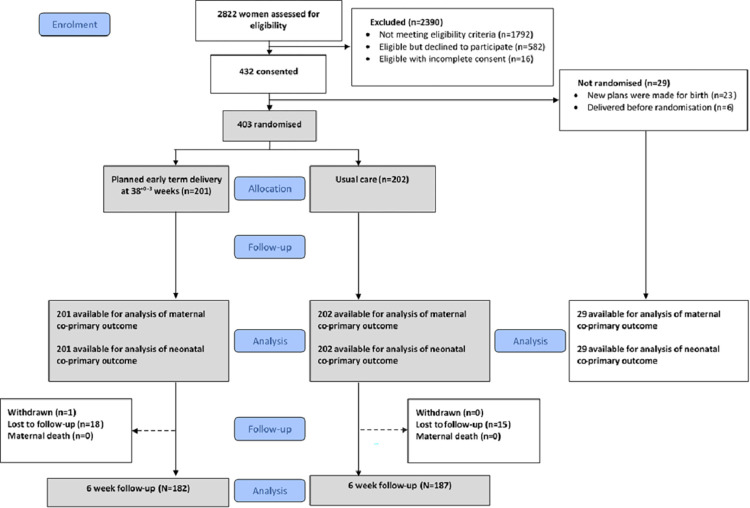
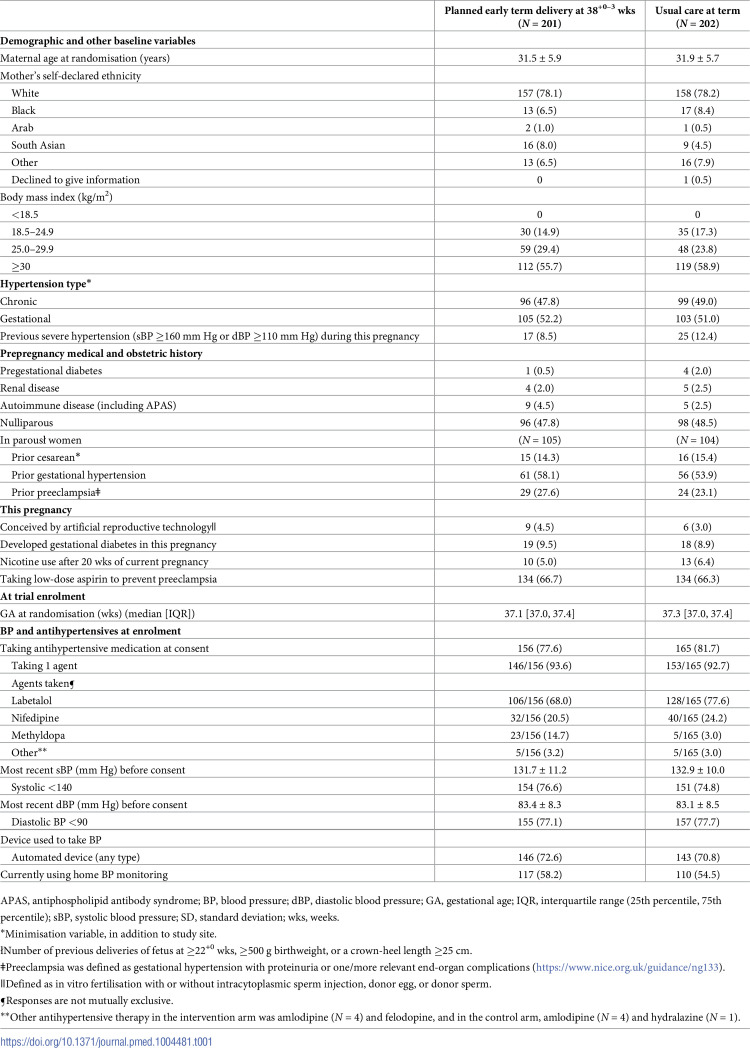
Methods and findings: This 50-centre, open-label, randomised trial in the United Kingdom included an economic analysis. WILL randomised women with chronic or gestational hypertension at 36 to 37 weeks and a singleton fetus, and who provided documented informed consent to "Planned early term birth at 38+0-3 weeks" (intervention) or "usual care at term" (control). The coprimary outcomes were "poor maternal outcome" (composite of severe hypertension, maternal death, or maternal morbidity; superiority hypothesis) and "neonatal care unit admission for ≥4 hours" (noninferiority hypothesis). The key secondary was cesarean. Follow-up was to 6 weeks postpartum. The planned sample size was 540/group. Analysis was by intention-to-treat. A total of 403 participants (37.3% of target) were randomised to the intervention (n = 201) or control group (n = 202), from 3 June 2019 to 19 December 2022, when the funder stopped the trial for delayed recruitment. In the intervention (versus control) group, losses to follow-up were 18/201 (9%) versus 15/202 (7%). In each group, maternal age was about 30 years, about one-fifth of women were from ethnic minorities, over half had obesity, approximately half had chronic hypertension, and most were on antihypertensives with normal blood pressure. In the intervention (versus control) group, birth was a median of 0.9 weeks earlier (38.4 [38.3 to 38.6] versus 39.3 [38.7 to 39.9] weeks). There was no evidence of a difference in "poor maternal outcome" (27/201 [13%] versus 24/202 [12%], respectively; adjusted risk ratio [aRR] 1.16, 95% confidence interval [CI] 0.72 to 1.87). For "neonatal care unit admission for ≥4 hours," the intervention was considered noninferior to the control as the adjusted risk difference (aRD) 95% CI upper bound did not cross the 8% prespecified noninferiority margin (14/201 [7%] versus 14/202 [7%], respectively; aRD 0.003, 95% CI -0.05 to +0.06), although event rates were lower-than-estimated. The intervention (versus control) was associated with no difference in cesarean (58/201 [29%] versus 72/202 [36%], respectively; aRR 0.81, 95% CI 0.61 to 1.08. There were no serious adverse events. Limitations include our smaller-than-planned sample size, and lower-than-anticipated event rates, so the findings may not be generalisable to where hypertension is not treated with antihypertensive therapy.
Conclusions: In this study, we observed that most women with chronic or gestational hypertension required labour induction, and planned birth at 38+0-3 weeks (versus usual care) resulted in birth an average of 6 days earlier, and no differences in poor maternal outcome or neonatal morbidity. Our findings provide reassurance about planned birth at 38+0-3 weeks as a clinical option for these women.
期刊介绍:
PLOS Medicine is a prominent platform for discussing and researching global health challenges. The journal covers a wide range of topics, including biomedical, environmental, social, and political factors affecting health. It prioritizes articles that contribute to clinical practice, health policy, or a better understanding of pathophysiology, ultimately aiming to improve health outcomes across different settings.
The journal is unwavering in its commitment to uphold the highest ethical standards in medical publishing. This includes actively managing and disclosing any conflicts of interest related to reporting, reviewing, and publishing. PLOS Medicine promotes transparency in the entire review and publication process. The journal also encourages data sharing and encourages the reuse of published work. Additionally, authors retain copyright for their work, and the publication is made accessible through Open Access with no restrictions on availability and dissemination.
PLOS Medicine takes measures to avoid conflicts of interest associated with advertising drugs and medical devices or engaging in the exclusive sale of reprints.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


