{"title":"封闭式与开放式重症监护病房对因急性腹部并发症需要紧急手术治疗的癌症患者死亡率的影响:韩国一项单中心回顾性研究。","authors":"Jae Hoon Lee, Jee Hee Kim, Ki Ho You, Won Ho Han","doi":"10.4266/acc.2024.00808","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In this study, we aimed to compare the in-hospital mortality of patients with cancer who experienced acute abdominal complications that required emergent surgery in open (treatment decisions made by the primary attending physician of the patient's admission department) versus closed (treatment decisions made by intensive care unit [ICU] intensivists) ICUs.</p><p><strong>Methods: </strong>This retrospective, single-center study enrolled patients with cancer admitted to the ICU before or after emergency surgery between November 2020 and September 2023. Univariate and logistic regression analyses were conducted to explore the associations between patient characteristics in the open and closed ICUs and in-hospital mortality.</p><p><strong>Results: </strong>Among the 100 patients (open ICU, 49; closed ICU, 51), 23 died during hospitalization. The closed ICU group had higher Acute Physiology and Chronic Health Evaluation (APACHE) II scores, vasopressor use, mechanical ventilation, and preoperative lactate levels and a shorter duration from diagnosis to ICU admission, surgery, and antibiotic administration than the open ICU group. Univariate analysis linked in-hospital mortality and APACHE II score, postoperative lactate levels, continuous renal replacement therapy (CRRT), and mechanical ventilation. Multivariate analysis revealed that in-hospital mortality rate increased with CRRT use and was lower in the closed ICU.</p><p><strong>Conclusions: </strong>Compared to an open ICU, a closed ICU was an independent factor in reducing in-hospital mortality through prompt and appropriate treatment.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":" ","pages":"554-564"},"PeriodicalIF":2.0000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11617842/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of closed- versus open-system intensive care units on mortality rates in patients with cancer requiring emergent surgical intervention for acute abdominal complications: a single-center retrospective study in Korea.\",\"authors\":\"Jae Hoon Lee, Jee Hee Kim, Ki Ho You, Won Ho Han\",\"doi\":\"10.4266/acc.2024.00808\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In this study, we aimed to compare the in-hospital mortality of patients with cancer who experienced acute abdominal complications that required emergent surgery in open (treatment decisions made by the primary attending physician of the patient's admission department) versus closed (treatment decisions made by intensive care unit [ICU] intensivists) ICUs.</p><p><strong>Methods: </strong>This retrospective, single-center study enrolled patients with cancer admitted to the ICU before or after emergency surgery between November 2020 and September 2023. Univariate and logistic regression analyses were conducted to explore the associations between patient characteristics in the open and closed ICUs and in-hospital mortality.</p><p><strong>Results: </strong>Among the 100 patients (open ICU, 49; closed ICU, 51), 23 died during hospitalization. The closed ICU group had higher Acute Physiology and Chronic Health Evaluation (APACHE) II scores, vasopressor use, mechanical ventilation, and preoperative lactate levels and a shorter duration from diagnosis to ICU admission, surgery, and antibiotic administration than the open ICU group. Univariate analysis linked in-hospital mortality and APACHE II score, postoperative lactate levels, continuous renal replacement therapy (CRRT), and mechanical ventilation. Multivariate analysis revealed that in-hospital mortality rate increased with CRRT use and was lower in the closed ICU.</p><p><strong>Conclusions: </strong>Compared to an open ICU, a closed ICU was an independent factor in reducing in-hospital mortality through prompt and appropriate treatment.</p>\",\"PeriodicalId\":44118,\"journal\":{\"name\":\"Acute and Critical Care\",\"volume\":\" \",\"pages\":\"554-564\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11617842/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acute and Critical Care\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4266/acc.2024.00808\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.2024.00808","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/25 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Effects of closed- versus open-system intensive care units on mortality rates in patients with cancer requiring emergent surgical intervention for acute abdominal complications: a single-center retrospective study in Korea.
Background: In this study, we aimed to compare the in-hospital mortality of patients with cancer who experienced acute abdominal complications that required emergent surgery in open (treatment decisions made by the primary attending physician of the patient's admission department) versus closed (treatment decisions made by intensive care unit [ICU] intensivists) ICUs.
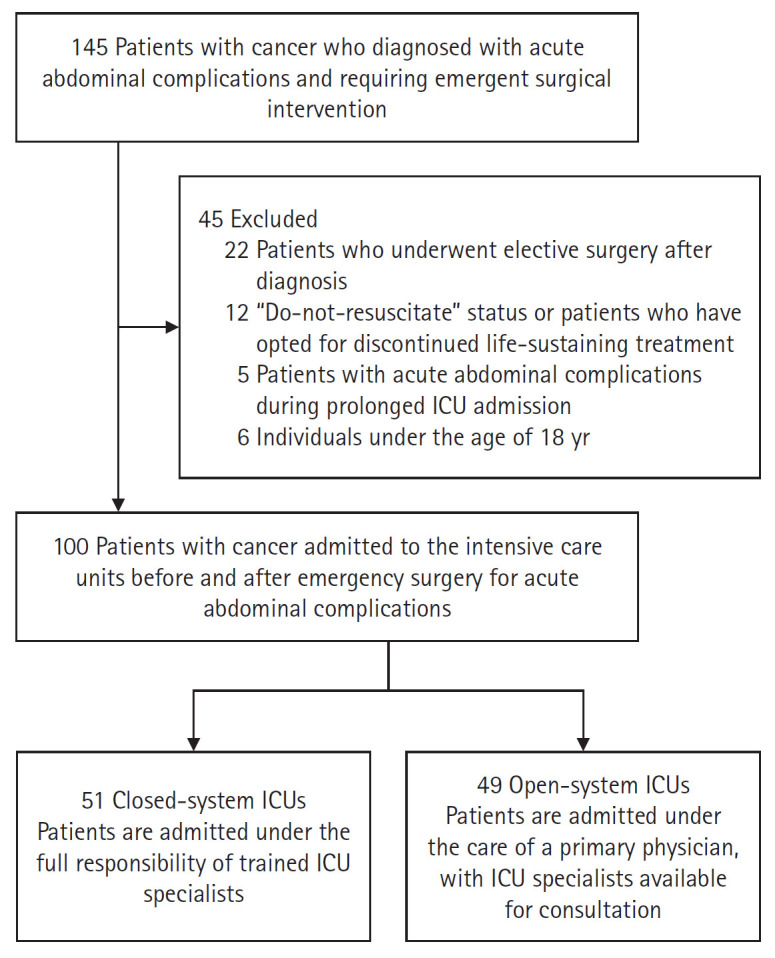
Methods: This retrospective, single-center study enrolled patients with cancer admitted to the ICU before or after emergency surgery between November 2020 and September 2023. Univariate and logistic regression analyses were conducted to explore the associations between patient characteristics in the open and closed ICUs and in-hospital mortality.
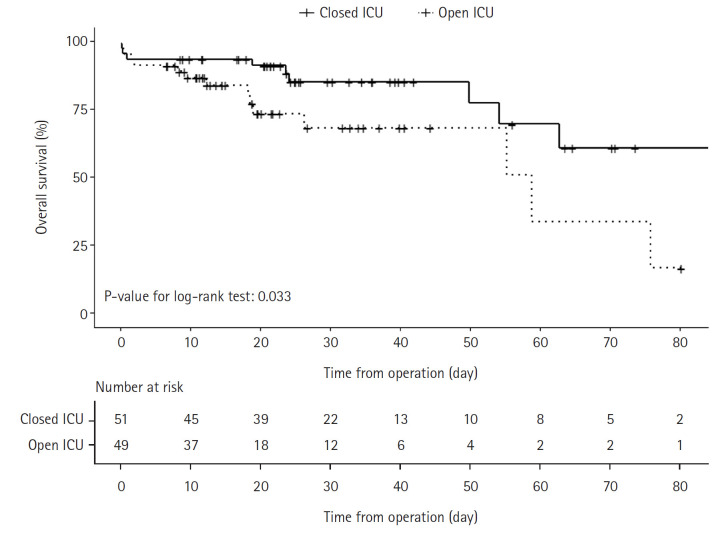
Results: Among the 100 patients (open ICU, 49; closed ICU, 51), 23 died during hospitalization. The closed ICU group had higher Acute Physiology and Chronic Health Evaluation (APACHE) II scores, vasopressor use, mechanical ventilation, and preoperative lactate levels and a shorter duration from diagnosis to ICU admission, surgery, and antibiotic administration than the open ICU group. Univariate analysis linked in-hospital mortality and APACHE II score, postoperative lactate levels, continuous renal replacement therapy (CRRT), and mechanical ventilation. Multivariate analysis revealed that in-hospital mortality rate increased with CRRT use and was lower in the closed ICU.
Conclusions: Compared to an open ICU, a closed ICU was an independent factor in reducing in-hospital mortality through prompt and appropriate treatment.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


