Osama Hallak, Karley Fischer, Shaina Ailawadi, Damian Valencia, Yan Yatsynovich, Raja Nazir, Brian Schwartz
{"title":"生物人工瓣膜断裂对瓣中瓣经导管主动脉瓣植入术跨瓣梯度的影响。","authors":"Osama Hallak, Karley Fischer, Shaina Ailawadi, Damian Valencia, Yan Yatsynovich, Raja Nazir, Brian Schwartz","doi":"10.14503/THIJ-23-8304","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Valve-in-valve (ViV) transcatheter aortic valve implantation (TAVI) is quickly becoming a routine and effective means by which to treat degenerated bioprosthetic valves. A known complication of ViV-TAVI is patient-prosthesis mismatch, which substantially affects survival. Bioprosthetic valve fracture is a method by which to reduce the risk of patient-prosthesis mismatch and post-ViV-TAVI transvalvular gradients. This study sought to determine the safety and efficacy of post-ViV-TAVI bioprosthetic valve fracture.</p><p><strong>Methods: </strong>Patients with a history of surgical aortic valve replacement undergoing ViV-TAVI bioprosthetic valve fracture (N = 25) at the corresponding institution from 2015 to 2022 were cataloged for a retrospective analysis. The implanted transcatheter valves were Medtronic Evolut R, Evolut PRO, and Evolut PRO+. Gradients were assessed before and after implantation and after fracturing using transthoracic echocardiogram.</p><p><strong>Results: </strong>The mean left ventricular ejection fraction of patients who underwent fracturing was 55.04%. The average (SD) peak and mean (SD) transvalvular gradients before the intervention were 68.17 (19.09) mm Hg and 38.98 (14.37) mm Hg, respectively. After ViV-TAVI, the same gradients were reduced to 27.25 (12.27) mm Hg and 15.63 (6.47) mm Hg, respectively. After bioprosthetic valve fracture, the gradients further decreased to 17.59 (7.93) mm Hg and 8.860 (3.334) mm Hg, respectively. The average reduction in peak gradient associated with fracturing was 12.07 mm Hg (95% CI, 5.73-18.41 mm Hg; <i>P</i> = .001). The average reduction in mean gradient associated with valve fracturing was 6.97 mm Hg (95% CI, 3.99-9.74 mm Hg; <i>P</i> < .001).</p><p><strong>Conclusion: </strong>Bioprosthetic valve fracture is a viable option for reducing residual transvalvular gradients after ViV-TAVI and should be considered in patients with elevated gradients (>20 mm Hg) or with concern for patient-prosthesis mismatch in patients who have an unacceptable risk for a redo sternotomy and surgical aortic valve replacement.</p>","PeriodicalId":48680,"journal":{"name":"Texas Heart Institute Journal","volume":"51 2","pages":"e238304"},"PeriodicalIF":0.9000,"publicationDate":"2024-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11584884/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of Bioprosthetic Valve Fracturing on Valve-in-Valve Transcatheter Aortic Valve Implantation Transvalvular Gradients.\",\"authors\":\"Osama Hallak, Karley Fischer, Shaina Ailawadi, Damian Valencia, Yan Yatsynovich, Raja Nazir, Brian Schwartz\",\"doi\":\"10.14503/THIJ-23-8304\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Valve-in-valve (ViV) transcatheter aortic valve implantation (TAVI) is quickly becoming a routine and effective means by which to treat degenerated bioprosthetic valves. A known complication of ViV-TAVI is patient-prosthesis mismatch, which substantially affects survival. Bioprosthetic valve fracture is a method by which to reduce the risk of patient-prosthesis mismatch and post-ViV-TAVI transvalvular gradients. This study sought to determine the safety and efficacy of post-ViV-TAVI bioprosthetic valve fracture.</p><p><strong>Methods: </strong>Patients with a history of surgical aortic valve replacement undergoing ViV-TAVI bioprosthetic valve fracture (N = 25) at the corresponding institution from 2015 to 2022 were cataloged for a retrospective analysis. The implanted transcatheter valves were Medtronic Evolut R, Evolut PRO, and Evolut PRO+. Gradients were assessed before and after implantation and after fracturing using transthoracic echocardiogram.</p><p><strong>Results: </strong>The mean left ventricular ejection fraction of patients who underwent fracturing was 55.04%. The average (SD) peak and mean (SD) transvalvular gradients before the intervention were 68.17 (19.09) mm Hg and 38.98 (14.37) mm Hg, respectively. After ViV-TAVI, the same gradients were reduced to 27.25 (12.27) mm Hg and 15.63 (6.47) mm Hg, respectively. After bioprosthetic valve fracture, the gradients further decreased to 17.59 (7.93) mm Hg and 8.860 (3.334) mm Hg, respectively. The average reduction in peak gradient associated with fracturing was 12.07 mm Hg (95% CI, 5.73-18.41 mm Hg; <i>P</i> = .001). The average reduction in mean gradient associated with valve fracturing was 6.97 mm Hg (95% CI, 3.99-9.74 mm Hg; <i>P</i> < .001).</p><p><strong>Conclusion: </strong>Bioprosthetic valve fracture is a viable option for reducing residual transvalvular gradients after ViV-TAVI and should be considered in patients with elevated gradients (>20 mm Hg) or with concern for patient-prosthesis mismatch in patients who have an unacceptable risk for a redo sternotomy and surgical aortic valve replacement.</p>\",\"PeriodicalId\":48680,\"journal\":{\"name\":\"Texas Heart Institute Journal\",\"volume\":\"51 2\",\"pages\":\"e238304\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-11-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11584884/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Texas Heart Institute Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14503/THIJ-23-8304\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Texas Heart Institute Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14503/THIJ-23-8304","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:瓣中瓣(ViV)经导管主动脉瓣植入术(TAVI)正迅速成为治疗退化的生物人工瓣膜的常规有效手段。ViV-TAVI的一个已知并发症是患者与人工瓣膜不匹配,这会严重影响存活率。生物人工瓣膜断裂是降低患者-人工瓣膜不匹配和ViV-TAVI术后跨瓣梯度风险的一种方法。本研究旨在确定ViV-TAVI术后生物瓣膜骨折的安全性和有效性:对2015年至2022年在相应机构接受ViV-TAVI生物人工瓣膜骨折手术的有主动脉瓣置换术史的患者(N = 25)进行编目,以进行回顾性分析。植入的经导管瓣膜为美敦力 Evolut R、Evolut PRO 和 Evolut PRO+。使用经胸超声心动图对植入前后和骨折后的瓣膜梯度进行评估:结果:接受骨折治疗的患者平均左心室射血分数为 55.04%。介入前的平均(标清)峰值和平均(标清)跨瓣梯度分别为 68.17 (19.09) mm Hg 和 38.98 (14.37) mm Hg。ViV-TAVI 术后,同样的梯度分别降至 27.25 (12.27) mm Hg 和 15.63 (6.47) mm Hg。生物瓣膜断裂后,阶差分别进一步降至17.59(7.93)毫米汞柱和8.860(3.334)毫米汞柱。与骨折相关的峰值阶差平均降低了 12.07 mm Hg(95% CI,5.73-18.41 mm Hg;P = .001)。与瓣膜骨折相关的平均梯度平均降低6.97毫米汞柱(95% CI,3.99-9.74毫米汞柱;P < .001):生物人工瓣膜骨折是降低ViV-TAVI术后残余跨瓣梯度的可行方案,对于梯度升高(>20毫米汞柱)的患者,或担心患者与人工瓣膜不匹配、重新进行胸骨切开术和外科主动脉瓣置换术的风险不可接受的患者,应考虑进行生物人工瓣膜骨折。
Effects of Bioprosthetic Valve Fracturing on Valve-in-Valve Transcatheter Aortic Valve Implantation Transvalvular Gradients.
Background: Valve-in-valve (ViV) transcatheter aortic valve implantation (TAVI) is quickly becoming a routine and effective means by which to treat degenerated bioprosthetic valves. A known complication of ViV-TAVI is patient-prosthesis mismatch, which substantially affects survival. Bioprosthetic valve fracture is a method by which to reduce the risk of patient-prosthesis mismatch and post-ViV-TAVI transvalvular gradients. This study sought to determine the safety and efficacy of post-ViV-TAVI bioprosthetic valve fracture.
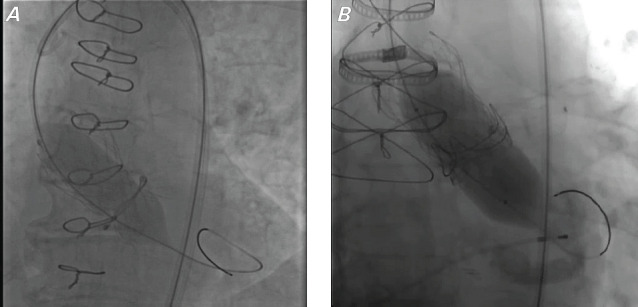
Methods: Patients with a history of surgical aortic valve replacement undergoing ViV-TAVI bioprosthetic valve fracture (N = 25) at the corresponding institution from 2015 to 2022 were cataloged for a retrospective analysis. The implanted transcatheter valves were Medtronic Evolut R, Evolut PRO, and Evolut PRO+. Gradients were assessed before and after implantation and after fracturing using transthoracic echocardiogram.
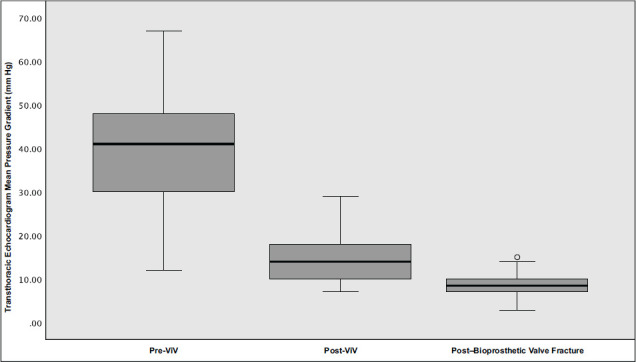
Results: The mean left ventricular ejection fraction of patients who underwent fracturing was 55.04%. The average (SD) peak and mean (SD) transvalvular gradients before the intervention were 68.17 (19.09) mm Hg and 38.98 (14.37) mm Hg, respectively. After ViV-TAVI, the same gradients were reduced to 27.25 (12.27) mm Hg and 15.63 (6.47) mm Hg, respectively. After bioprosthetic valve fracture, the gradients further decreased to 17.59 (7.93) mm Hg and 8.860 (3.334) mm Hg, respectively. The average reduction in peak gradient associated with fracturing was 12.07 mm Hg (95% CI, 5.73-18.41 mm Hg; P = .001). The average reduction in mean gradient associated with valve fracturing was 6.97 mm Hg (95% CI, 3.99-9.74 mm Hg; P < .001).
Conclusion: Bioprosthetic valve fracture is a viable option for reducing residual transvalvular gradients after ViV-TAVI and should be considered in patients with elevated gradients (>20 mm Hg) or with concern for patient-prosthesis mismatch in patients who have an unacceptable risk for a redo sternotomy and surgical aortic valve replacement.
期刊介绍:
For more than 45 years, the Texas Heart Institute Journal has been published by the Texas Heart Institute as part of its medical education program. Our bimonthly peer-reviewed journal enjoys a global audience of physicians, scientists, and healthcare professionals who are contributing to the prevention, diagnosis, and treatment of cardiovascular disease.
The Journal was printed under the name of Cardiovascular Diseases from 1974 through 1981 (ISSN 0093-3546). The name was changed to Texas Heart Institute Journal in 1982 and was printed through 2013 (ISSN 0730-2347). In 2014, the Journal moved to online-only publication. It is indexed by Index Medicus/MEDLINE and by other indexing and abstracting services worldwide. Our full archive is available at PubMed Central.
The Journal invites authors to submit these article types for review:
-Clinical Investigations-
Laboratory Investigations-
Reviews-
Techniques-
Coronary Anomalies-
History of Medicine-
Case Reports/Case Series (Submission Fee: $70.00 USD)-
Images in Cardiovascular Medicine (Submission Fee: $35.00 USD)-
Guest Editorials-
Peabody’s Corner-
Letters to the Editor

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


