Massimo Martino, Martina Pitea, Annalisa Sgarlata, Ilaria Maria Delfino, Francesca Cogliandro, Anna Scopelliti, Violetta Marafioti, Simona Polimeni, Gaetana Porto, Giorgia Policastro, Giovanna Utano, Maria Pellicano, Giovanni Leanza, Caterina Alati
{"title":"用于治疗骨髓纤维化的治疗策略:最新技术。","authors":"Massimo Martino, Martina Pitea, Annalisa Sgarlata, Ilaria Maria Delfino, Francesca Cogliandro, Anna Scopelliti, Violetta Marafioti, Simona Polimeni, Gaetana Porto, Giorgia Policastro, Giovanna Utano, Maria Pellicano, Giovanni Leanza, Caterina Alati","doi":"10.3390/hematolrep16040067","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Current drug therapy for myelofibrosis does not alter the natural course of the disease or prolong survival, and allogeneic stem cell transplantation is the only curative treatment modality. For over a decade, the Janus kinase (JAK) inhibitor ruxolitinib has been the standard of care. More recently, newer-generation JAK inhibitors have joined the ranks of accepted treatment options.</p><p><strong>Objectives: </strong>The primary goal of treatment is to reduce spleen size and minimize disease-related symptoms. Prognostic scoring systems are used to designate patients as being at lower or higher risk. For transplant-eligible patients, transplant is offered to those with a bridge of a JAK inhibitor; patients who are not eligible for transplant are usually offered long-term therapy with a JAK inhibitor. Limited disease-modifying activity, dose-limiting cytopenias, and other adverse effects have contributed to discontinuation of JAK inhibitor treatment.</p><p><strong>Conclusions: </strong>Novel JAK inhibitors and combination approaches are currently being explored to overcome these shortcomings. Further research will be essential to establish optimal therapeutic approaches in first-line and subsequent treatments.</p>","PeriodicalId":12829,"journal":{"name":"Hematology Reports","volume":"16 4","pages":"698-713"},"PeriodicalIF":1.2000,"publicationDate":"2024-10-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11587016/pdf/","citationCount":"0","resultStr":"{\"title\":\"Treatment Strategies Used in Treating Myelofibrosis: State of the Art.\",\"authors\":\"Massimo Martino, Martina Pitea, Annalisa Sgarlata, Ilaria Maria Delfino, Francesca Cogliandro, Anna Scopelliti, Violetta Marafioti, Simona Polimeni, Gaetana Porto, Giorgia Policastro, Giovanna Utano, Maria Pellicano, Giovanni Leanza, Caterina Alati\",\"doi\":\"10.3390/hematolrep16040067\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Current drug therapy for myelofibrosis does not alter the natural course of the disease or prolong survival, and allogeneic stem cell transplantation is the only curative treatment modality. For over a decade, the Janus kinase (JAK) inhibitor ruxolitinib has been the standard of care. More recently, newer-generation JAK inhibitors have joined the ranks of accepted treatment options.</p><p><strong>Objectives: </strong>The primary goal of treatment is to reduce spleen size and minimize disease-related symptoms. Prognostic scoring systems are used to designate patients as being at lower or higher risk. For transplant-eligible patients, transplant is offered to those with a bridge of a JAK inhibitor; patients who are not eligible for transplant are usually offered long-term therapy with a JAK inhibitor. Limited disease-modifying activity, dose-limiting cytopenias, and other adverse effects have contributed to discontinuation of JAK inhibitor treatment.</p><p><strong>Conclusions: </strong>Novel JAK inhibitors and combination approaches are currently being explored to overcome these shortcomings. Further research will be essential to establish optimal therapeutic approaches in first-line and subsequent treatments.</p>\",\"PeriodicalId\":12829,\"journal\":{\"name\":\"Hematology Reports\",\"volume\":\"16 4\",\"pages\":\"698-713\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-10-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11587016/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hematology Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/hematolrep16040067\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hematology Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/hematolrep16040067","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:目前骨髓纤维化的药物治疗无法改变疾病的自然病程或延长存活时间,异基因干细胞移植是唯一可治愈的治疗方式。十多年来,Janus激酶(JAK)抑制剂鲁索利替尼一直是标准疗法。最近,新一代的JAK抑制剂也加入了公认的治疗方案行列:治疗的主要目标是缩小脾脏大小并尽量减轻疾病相关症状。预后评分系统用于将患者划分为低风险或高风险。对于符合移植条件的患者,可通过使用 JAK 抑制剂进行桥接来进行移植;对于不符合移植条件的患者,通常可使用 JAK 抑制剂进行长期治疗。有限的疾病改变活性、剂量限制性细胞减少症和其他不良反应导致了JAK抑制剂治疗的中断:结论:目前正在探索新型 JAK 抑制剂和联合疗法,以克服这些不足。进一步的研究对于确定一线治疗和后续治疗的最佳治疗方法至关重要。
Treatment Strategies Used in Treating Myelofibrosis: State of the Art.
Background: Current drug therapy for myelofibrosis does not alter the natural course of the disease or prolong survival, and allogeneic stem cell transplantation is the only curative treatment modality. For over a decade, the Janus kinase (JAK) inhibitor ruxolitinib has been the standard of care. More recently, newer-generation JAK inhibitors have joined the ranks of accepted treatment options.
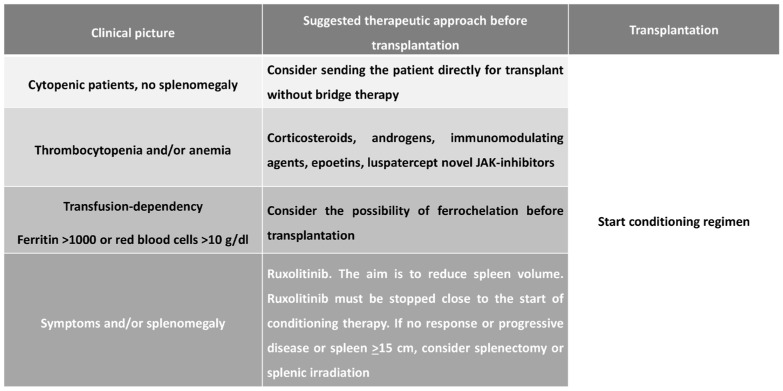
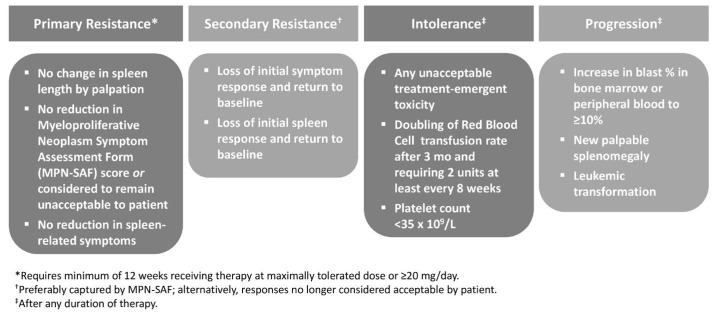
Objectives: The primary goal of treatment is to reduce spleen size and minimize disease-related symptoms. Prognostic scoring systems are used to designate patients as being at lower or higher risk. For transplant-eligible patients, transplant is offered to those with a bridge of a JAK inhibitor; patients who are not eligible for transplant are usually offered long-term therapy with a JAK inhibitor. Limited disease-modifying activity, dose-limiting cytopenias, and other adverse effects have contributed to discontinuation of JAK inhibitor treatment.
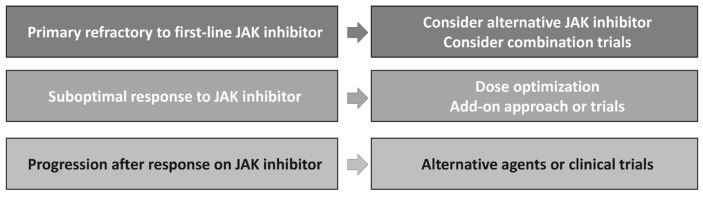
Conclusions: Novel JAK inhibitors and combination approaches are currently being explored to overcome these shortcomings. Further research will be essential to establish optimal therapeutic approaches in first-line and subsequent treatments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


