Xiangqing Sun, Zhengyi Chen, Gregory S Cooper, Nathan A Berger, Claudia Coulton, Li Li
{"title":"晚期结直肠肿瘤的风险预测因种族和社区社会经济地位而异。","authors":"Xiangqing Sun, Zhengyi Chen, Gregory S Cooper, Nathan A Berger, Claudia Coulton, Li Li","doi":"10.1136/fmch-2024-002892","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Neighbourhood deprivation increases the risk of colorectal neoplasia and contributes to racial disparities observed in this disease. Developing race-specific advanced colorectal neoplasia (ACN) prediction models that include neighbourhood socioeconomic status has the potential to improve the accuracy of prediction.</p><p><strong>Methods: </strong>The study includes 1457 European Americans (EAs) and 936 African Americans (AAs) aged 50-80 years undergoing screening colonoscopy. Race-specific ACN risk prediction models were developed for EAs and AAs, respectively. Area Deprivation Index (ADI), derived from 17 variables of neighbourhood socioeconomic status, was evaluated by adding it to the ACN risk prediction models. Prediction accuracy was evaluated by concordance statistic (C-statistic) for discrimination and Hosmer-Lemeshow goodness-of-fit test for calibration.</p><p><strong>Results: </strong>With fewer predictors, the EA-specific and AA-specific prediction models had better prediction accuracy in the corresponding race/ethnic subpopulation than the overall model. Compared with the overall model which had poor calibration (<i>P</i> <sub>Calibration</sub>=0.053 in the whole population and <i>P</i> <sub>Calibration</sub>=0.011 in AAs), the EA model had C-statistic of 0.655 (95% CI 0.594 to 0.717) and <i>P</i> <sub>Calibration</sub>=0.663; and the AA model had C-statistic of 0.637 ((95% CI 0.572 to 0.702) and <i>P</i> <sub>Calibration</sub>=0.810. ADI was a significant predictor of ACN in EAs (OR=1.24 ((95% CI 1.03 to 1.50), <i>P</i>=0.029), but not in AAs (OR=1.07 ((95% CI 0.89 to 1.28), <i>P</i>=0.487). Adding ADI to the EA-specific ACN prediction model substantially improved ACN calibration accuracy of the prediction across area deprivation groups (<i>P</i> <sub>Calibration</sub>=0.924 with ADI vs <i>P</i> <sub>Calibration</sub>=0.140 without ADI) in EAs.</p><p><strong>Conclusions: </strong>Neighbourhood socioeconomic status is an important factor to consider in ACN risk prediction modeling. Moreover, non-race-specific prediction models have poor generalisability. Race-specific prediction models incorporating neighbourhood socioeconomic factors are needed to improve ACN prediction accuracy.</p>","PeriodicalId":44590,"journal":{"name":"Family Medicine and Community Health","volume":"12 Suppl 2","pages":""},"PeriodicalIF":4.3000,"publicationDate":"2024-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11141178/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk prediction of advanced colorectal neoplasia varies by race and neighbourhood socioeconomic status.\",\"authors\":\"Xiangqing Sun, Zhengyi Chen, Gregory S Cooper, Nathan A Berger, Claudia Coulton, Li Li\",\"doi\":\"10.1136/fmch-2024-002892\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Neighbourhood deprivation increases the risk of colorectal neoplasia and contributes to racial disparities observed in this disease. Developing race-specific advanced colorectal neoplasia (ACN) prediction models that include neighbourhood socioeconomic status has the potential to improve the accuracy of prediction.</p><p><strong>Methods: </strong>The study includes 1457 European Americans (EAs) and 936 African Americans (AAs) aged 50-80 years undergoing screening colonoscopy. Race-specific ACN risk prediction models were developed for EAs and AAs, respectively. Area Deprivation Index (ADI), derived from 17 variables of neighbourhood socioeconomic status, was evaluated by adding it to the ACN risk prediction models. Prediction accuracy was evaluated by concordance statistic (C-statistic) for discrimination and Hosmer-Lemeshow goodness-of-fit test for calibration.</p><p><strong>Results: </strong>With fewer predictors, the EA-specific and AA-specific prediction models had better prediction accuracy in the corresponding race/ethnic subpopulation than the overall model. Compared with the overall model which had poor calibration (<i>P</i> <sub>Calibration</sub>=0.053 in the whole population and <i>P</i> <sub>Calibration</sub>=0.011 in AAs), the EA model had C-statistic of 0.655 (95% CI 0.594 to 0.717) and <i>P</i> <sub>Calibration</sub>=0.663; and the AA model had C-statistic of 0.637 ((95% CI 0.572 to 0.702) and <i>P</i> <sub>Calibration</sub>=0.810. ADI was a significant predictor of ACN in EAs (OR=1.24 ((95% CI 1.03 to 1.50), <i>P</i>=0.029), but not in AAs (OR=1.07 ((95% CI 0.89 to 1.28), <i>P</i>=0.487). Adding ADI to the EA-specific ACN prediction model substantially improved ACN calibration accuracy of the prediction across area deprivation groups (<i>P</i> <sub>Calibration</sub>=0.924 with ADI vs <i>P</i> <sub>Calibration</sub>=0.140 without ADI) in EAs.</p><p><strong>Conclusions: </strong>Neighbourhood socioeconomic status is an important factor to consider in ACN risk prediction modeling. Moreover, non-race-specific prediction models have poor generalisability. Race-specific prediction models incorporating neighbourhood socioeconomic factors are needed to improve ACN prediction accuracy.</p>\",\"PeriodicalId\":44590,\"journal\":{\"name\":\"Family Medicine and Community Health\",\"volume\":\"12 Suppl 2\",\"pages\":\"\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-05-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11141178/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Family Medicine and Community Health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/fmch-2024-002892\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PRIMARY HEALTH CARE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Family Medicine and Community Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/fmch-2024-002892","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 0
摘要
目的:社区贫困会增加罹患结直肠肿瘤的风险,并导致该疾病的种族差异。开发包含邻里社会经济状况的种族特异性晚期结直肠肿瘤(ACN)预测模型有可能提高预测的准确性:研究对象包括接受结肠镜筛查的 1457 名欧洲裔美国人(EAs)和 936 名 50-80 岁非裔美国人(AAs)。分别为欧裔美国人和非裔美国人建立了种族特异性 ACN 风险预测模型。地区贫困指数 (Area Deprivation Index, ADI) 由 17 个邻里社会经济状况变量得出,通过将其添加到 ACN 风险预测模型中进行评估。预测的准确性通过判别的一致性统计量(C统计量)和校准的Hosmer-Lemeshow拟合优度检验进行评估:结果:在预测因子较少的情况下,EA-特异性和 AA-特异性预测模型对相应种族/族裔亚群的预测准确性优于总体模型。EA模型的C统计量为0.655(95% CI为0.594至0.717),P校准值为0.663;AA模型的C统计量为0.637(95% CI为0.572至0.702),P校准值为0.810。在 EA 中,ADI 是 ACN 的重要预测因子(OR=1.24((95% CI 1.03 至 1.50),P=0.029),但在 AA 中不是(OR=1.07((95% CI 0.89 至 1.28),P=0.487)。在EA特异性ACN预测模型中加入ADI,大大提高了EA各地区贫困组ACN校准预测的准确性(有ADI时P校准=0.924,无ADI时P校准=0.140):结论:邻里社会经济状况是 ACN 风险预测模型中需要考虑的一个重要因素。此外,非种族特异性预测模型的普遍性较差。需要建立包含邻里社会经济因素的种族特异性预测模型,以提高ACN预测的准确性。
Risk prediction of advanced colorectal neoplasia varies by race and neighbourhood socioeconomic status.
Objective: Neighbourhood deprivation increases the risk of colorectal neoplasia and contributes to racial disparities observed in this disease. Developing race-specific advanced colorectal neoplasia (ACN) prediction models that include neighbourhood socioeconomic status has the potential to improve the accuracy of prediction.
Methods: The study includes 1457 European Americans (EAs) and 936 African Americans (AAs) aged 50-80 years undergoing screening colonoscopy. Race-specific ACN risk prediction models were developed for EAs and AAs, respectively. Area Deprivation Index (ADI), derived from 17 variables of neighbourhood socioeconomic status, was evaluated by adding it to the ACN risk prediction models. Prediction accuracy was evaluated by concordance statistic (C-statistic) for discrimination and Hosmer-Lemeshow goodness-of-fit test for calibration.
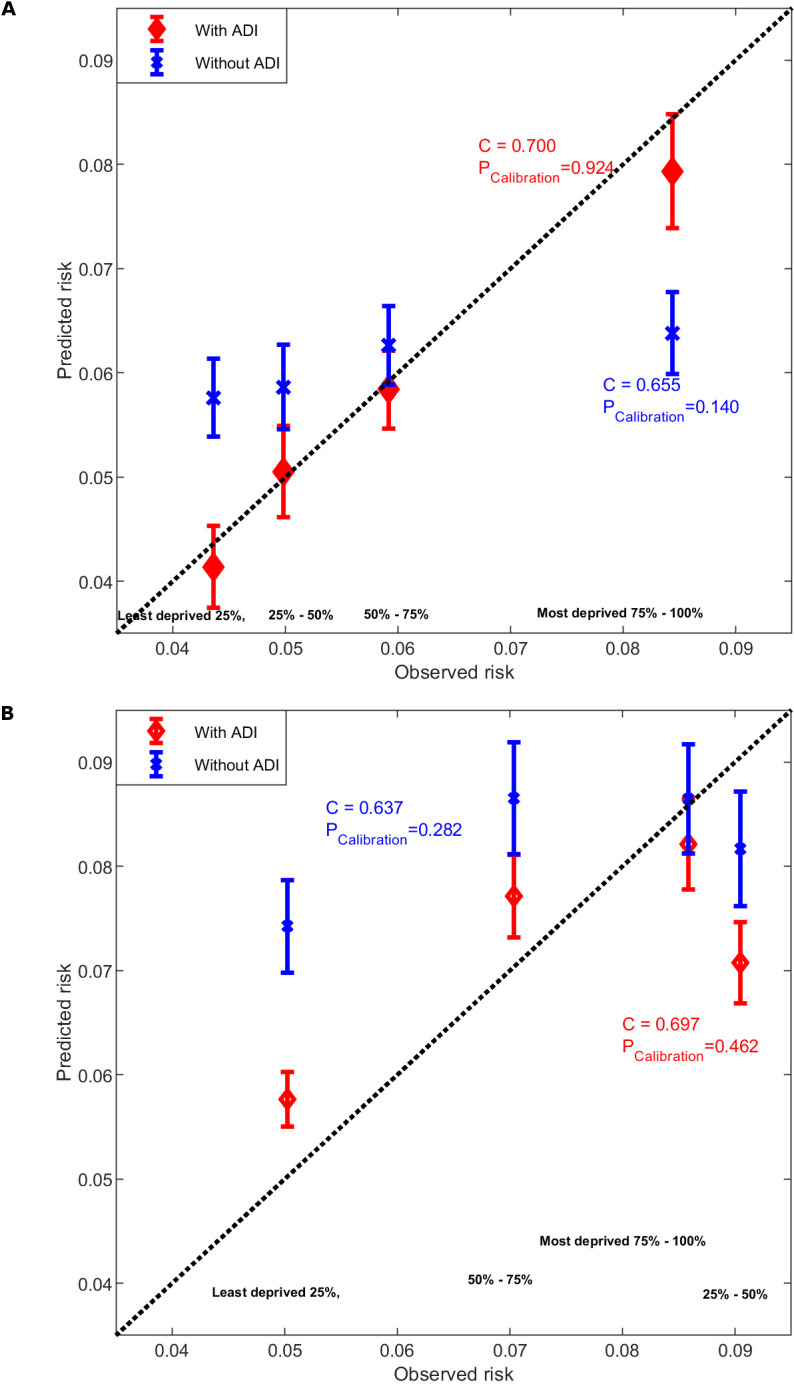
Results: With fewer predictors, the EA-specific and AA-specific prediction models had better prediction accuracy in the corresponding race/ethnic subpopulation than the overall model. Compared with the overall model which had poor calibration (PCalibration=0.053 in the whole population and PCalibration=0.011 in AAs), the EA model had C-statistic of 0.655 (95% CI 0.594 to 0.717) and PCalibration=0.663; and the AA model had C-statistic of 0.637 ((95% CI 0.572 to 0.702) and PCalibration=0.810. ADI was a significant predictor of ACN in EAs (OR=1.24 ((95% CI 1.03 to 1.50), P=0.029), but not in AAs (OR=1.07 ((95% CI 0.89 to 1.28), P=0.487). Adding ADI to the EA-specific ACN prediction model substantially improved ACN calibration accuracy of the prediction across area deprivation groups (PCalibration=0.924 with ADI vs PCalibration=0.140 without ADI) in EAs.
Conclusions: Neighbourhood socioeconomic status is an important factor to consider in ACN risk prediction modeling. Moreover, non-race-specific prediction models have poor generalisability. Race-specific prediction models incorporating neighbourhood socioeconomic factors are needed to improve ACN prediction accuracy.
期刊介绍:
Family Medicine and Community Health (FMCH) is a peer-reviewed, open-access journal focusing on the topics of family medicine, general practice and community health. FMCH strives to be a leading international journal that promotes ‘Health Care for All’ through disseminating novel knowledge and best practices in primary care, family medicine, and community health. FMCH publishes original research, review, methodology, commentary, reflection, and case-study from the lens of population health. FMCH’s Asian Focus section features reports of family medicine development in the Asia-pacific region. FMCH aims to be an exemplary forum for the timely communication of medical knowledge and skills with the goal of promoting improved health care through the practice of family and community-based medicine globally. FMCH aims to serve a diverse audience including researchers, educators, policymakers and leaders of family medicine and community health. We also aim to provide content relevant for researchers working on population health, epidemiology, public policy, disease control and management, preventative medicine and disease burden. FMCH does not impose any article processing charges (APC) or submission charges.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


