Jakob Kjølby Eika, Kasper Bonnesen, Lars Pedersen, Vera Ehrenstein, Henrik Toft Sørensen, Morten Schmidt
{"title":"布洛芬治疗急性心包炎及相关心血管风险:丹麦全国人口队列研究》。","authors":"Jakob Kjølby Eika, Kasper Bonnesen, Lars Pedersen, Vera Ehrenstein, Henrik Toft Sørensen, Morten Schmidt","doi":"10.2147/CLEP.S483553","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Ibuprofen is used to treat acute pericarditis, but high-dose ibuprofen has also been associated with increased cardiovascular risks. We examined the cardiovascular safety of using ibuprofen for acute pericarditis.</p><p><strong>Patients and methods: </strong>A Danish nationwide, population-based cohort study including patients <i>≥</i>18 years with first-time acute pericarditis (n=12,381) during 1996-2020 was conducted. Ibuprofen use was modelled in two ways: First, we considered patients exposed based on the tablet strength of their first ibuprofen filling (a proxy for an <i>intention-to-treat</i> analysis). Second, we considered patients exposed in a time-varying manner (a proxy for an <i>as-treated</i> analysis). The primary outcome of major adverse cardiovascular events (MACE) was a composite of myocardial infarction, ischemic stroke, congestive heart failure, and cardiovascular death.</p><p><strong>Results: </strong>In the <i>intention-to-treat</i> analysis, the 1-year risk of MACE was 1.37% (95% confidence interval [CI]: 1.03-1.79) for ibuprofen initiators and 4.32% (95% CI: 3.89-4.78) for non-initiators. Compared with non-initiators within 1-year follow-up, the adjusted hazard ratio for MACE was 0.75 (95% CI: 0.67-0.85) for initiators overall, 0.38 (95% CI: 0.28-0.52) for initiators of >400 mg tablets, and 0.87 (95% CI: 0.76-0.99) for initiators of ≤400 mg tablets. In the <i>as-treated</i> analysis, compared with no use, the hazard ratio associated with ibuprofen use was 0.69 (95% CI: 0.54-0.89) for MACE, 0.82 (95% CI: 0.54-1.26) for myocardial infarction, 0.74 (95% CI: 0.45-1.22) for ischemic stroke, 0.67 (95% CI: 0.47-0.96) for congestive heart failure, and 0.60 (95% CI: 0.31-1.17) for cardiovascular death.</p><p><strong>Conclusion: </strong>Ibuprofen use for acute pericarditis was not associated with increased cardiovascular risks, supporting its safety in current practice.</p>","PeriodicalId":10362,"journal":{"name":"Clinical Epidemiology","volume":"16 ","pages":"793-802"},"PeriodicalIF":3.2000,"publicationDate":"2024-11-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11572456/pdf/","citationCount":"0","resultStr":"{\"title\":\"Ibuprofen for Acute Pericarditis and Associated Cardiovascular Risks: A Danish Nationwide, Population-Based Cohort Study.\",\"authors\":\"Jakob Kjølby Eika, Kasper Bonnesen, Lars Pedersen, Vera Ehrenstein, Henrik Toft Sørensen, Morten Schmidt\",\"doi\":\"10.2147/CLEP.S483553\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Ibuprofen is used to treat acute pericarditis, but high-dose ibuprofen has also been associated with increased cardiovascular risks. We examined the cardiovascular safety of using ibuprofen for acute pericarditis.</p><p><strong>Patients and methods: </strong>A Danish nationwide, population-based cohort study including patients <i>≥</i>18 years with first-time acute pericarditis (n=12,381) during 1996-2020 was conducted. Ibuprofen use was modelled in two ways: First, we considered patients exposed based on the tablet strength of their first ibuprofen filling (a proxy for an <i>intention-to-treat</i> analysis). Second, we considered patients exposed in a time-varying manner (a proxy for an <i>as-treated</i> analysis). The primary outcome of major adverse cardiovascular events (MACE) was a composite of myocardial infarction, ischemic stroke, congestive heart failure, and cardiovascular death.</p><p><strong>Results: </strong>In the <i>intention-to-treat</i> analysis, the 1-year risk of MACE was 1.37% (95% confidence interval [CI]: 1.03-1.79) for ibuprofen initiators and 4.32% (95% CI: 3.89-4.78) for non-initiators. Compared with non-initiators within 1-year follow-up, the adjusted hazard ratio for MACE was 0.75 (95% CI: 0.67-0.85) for initiators overall, 0.38 (95% CI: 0.28-0.52) for initiators of >400 mg tablets, and 0.87 (95% CI: 0.76-0.99) for initiators of ≤400 mg tablets. In the <i>as-treated</i> analysis, compared with no use, the hazard ratio associated with ibuprofen use was 0.69 (95% CI: 0.54-0.89) for MACE, 0.82 (95% CI: 0.54-1.26) for myocardial infarction, 0.74 (95% CI: 0.45-1.22) for ischemic stroke, 0.67 (95% CI: 0.47-0.96) for congestive heart failure, and 0.60 (95% CI: 0.31-1.17) for cardiovascular death.</p><p><strong>Conclusion: </strong>Ibuprofen use for acute pericarditis was not associated with increased cardiovascular risks, supporting its safety in current practice.</p>\",\"PeriodicalId\":10362,\"journal\":{\"name\":\"Clinical Epidemiology\",\"volume\":\"16 \",\"pages\":\"793-802\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2024-11-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11572456/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Epidemiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/CLEP.S483553\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CLEP.S483553","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Ibuprofen for Acute Pericarditis and Associated Cardiovascular Risks: A Danish Nationwide, Population-Based Cohort Study.
Purpose: Ibuprofen is used to treat acute pericarditis, but high-dose ibuprofen has also been associated with increased cardiovascular risks. We examined the cardiovascular safety of using ibuprofen for acute pericarditis.
Patients and methods: A Danish nationwide, population-based cohort study including patients ≥18 years with first-time acute pericarditis (n=12,381) during 1996-2020 was conducted. Ibuprofen use was modelled in two ways: First, we considered patients exposed based on the tablet strength of their first ibuprofen filling (a proxy for an intention-to-treat analysis). Second, we considered patients exposed in a time-varying manner (a proxy for an as-treated analysis). The primary outcome of major adverse cardiovascular events (MACE) was a composite of myocardial infarction, ischemic stroke, congestive heart failure, and cardiovascular death.
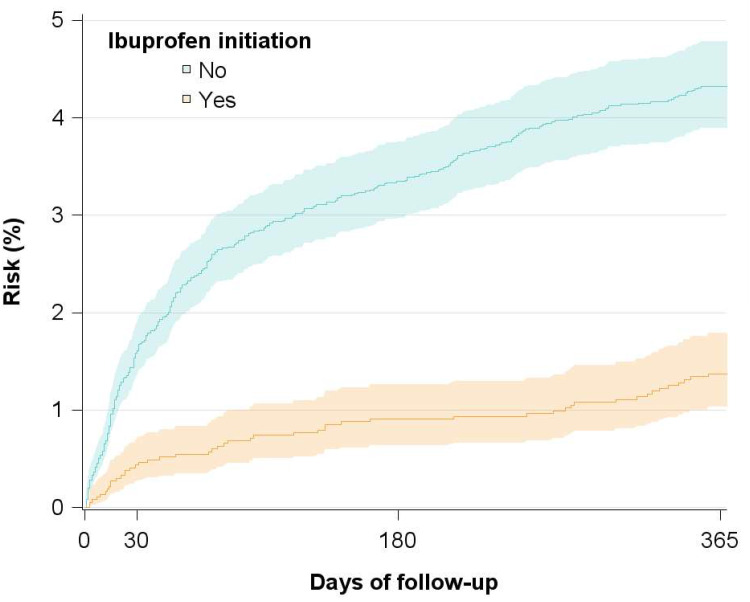
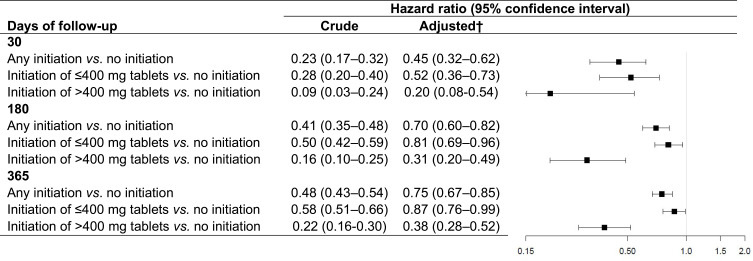
Results: In the intention-to-treat analysis, the 1-year risk of MACE was 1.37% (95% confidence interval [CI]: 1.03-1.79) for ibuprofen initiators and 4.32% (95% CI: 3.89-4.78) for non-initiators. Compared with non-initiators within 1-year follow-up, the adjusted hazard ratio for MACE was 0.75 (95% CI: 0.67-0.85) for initiators overall, 0.38 (95% CI: 0.28-0.52) for initiators of >400 mg tablets, and 0.87 (95% CI: 0.76-0.99) for initiators of ≤400 mg tablets. In the as-treated analysis, compared with no use, the hazard ratio associated with ibuprofen use was 0.69 (95% CI: 0.54-0.89) for MACE, 0.82 (95% CI: 0.54-1.26) for myocardial infarction, 0.74 (95% CI: 0.45-1.22) for ischemic stroke, 0.67 (95% CI: 0.47-0.96) for congestive heart failure, and 0.60 (95% CI: 0.31-1.17) for cardiovascular death.
Conclusion: Ibuprofen use for acute pericarditis was not associated with increased cardiovascular risks, supporting its safety in current practice.
期刊介绍:
Clinical Epidemiology is an international, peer reviewed, open access journal. Clinical Epidemiology focuses on the application of epidemiological principles and questions relating to patients and clinical care in terms of prevention, diagnosis, prognosis, and treatment.
Clinical Epidemiology welcomes papers covering these topics in form of original research and systematic reviews.
Clinical Epidemiology has a special interest in international electronic medical patient records and other routine health care data, especially as applied to safety of medical interventions, clinical utility of diagnostic procedures, understanding short- and long-term clinical course of diseases, clinical epidemiological and biostatistical methods, and systematic reviews.
When considering submission of a paper utilizing publicly-available data, authors should ensure that such studies add significantly to the body of knowledge and that they use appropriate validated methods for identifying health outcomes.
The journal has launched special series describing existing data sources for clinical epidemiology, international health care systems and validation studies of algorithms based on databases and registries.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


