{"title":"创伤患者排除胸腰椎骨折的临床诊断工具。","authors":"Sajid Atique, Ahammed Mekkodathil, Tariq Siddiqui, Saji Mathradikkal, Khalid Ahmed, Mushreq Al-Ani, Ahad Kanbar, Abubaker Alaieb, Suhail Hakim, Basil Younis, Ahmed Ajaj, Aldwin Guerrero, Maarij Masood, Sherwan Khoschnau, Abdel Aziz Hammo, Nuri Abdurraheim, Husham Abdelrahman, Ruben Peralta, Syed Nabir, Shatha Al-Hilli, Ayman El-Menyar, Hassan Al-Thani","doi":"10.4103/jets.jets_145_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The primary objective of this study was to assess the effectiveness of the clinical decision tool (CDT) in trauma patients, providing a comparable ability to rule out thoracolumbar (TL) fractures as traditional imaging methods. The goal is to facilitate early clearance of the TL spine without an immediate requirement for radiological tests, thereby minimizing unnecessary utilization of TL-spine imaging.</p><p><strong>Methods: </strong>A prospective, observational study was conducted on trauma patients with suspected TL injury. To achieve early TL clearance, the CDT assessed criteria such as absence of pain, tenderness, and pain-free axial movement and flexion. The study enrolled alert trauma patients with thoracic and/or lumbar spine injuries, defined by the Glasgow Coma Scale of 15. The study excluded patients not aligning with CDT criteria, such as those who received intravenous opioid analgesia within 4 h and those unable to stand due to suspected pelvic or lower limb injuries.</p><p><strong>Results: </strong>Following the completion of the CDT steps, there were 31 true negative cases, signifying the absence of TL fractures according to both CDT and imaging studies. The sensitivity of the CDT was 99.38% (95% confidence interval [CI]: 96.59%-99.98%), specificity 9.1% (95% CI: 6.30%-12.73%), negative predictive value (NPV) 96.87% (95% CI: 81.02%-99.56%), positive predictive value (PPV) 34.19% (95% CI: 33.38%-35.00%), negative likelihood ratio (LHR) 0.07 (95% CI: 0.01-0.49), and positive LHR 1.09 (95% CI: 1.06-1.13). The sensitivity, specificity, NPV, PPV, negative LHR, and positive LHR varied with each step in the CDT. Notably, the overall sensitivity was high; however, the stepwise sensitivity decreased, albeit with an improvement in specificity with each further step in the tool. The overall sensitivity in the study cohort (<i>n</i> = 500) was high; however, the stepwise sensitivity decreased, albeit with an improvement in the specificity.</p><p><strong>Conclusions: </strong>The CDT to rule out TL fracture is a feasible bedside stepwise tool in fully awake trauma patients after a thorough clinical neurological examination on arrival. The tool could help Level II or III trauma centers avoid secondary triage to the higher center.</p>","PeriodicalId":15692,"journal":{"name":"Journal of Emergencies, Trauma, and Shock","volume":"17 3","pages":"159-165"},"PeriodicalIF":0.7000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11563237/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diagnostic Clinical Tool in Trauma Patients to Rule out Thoracolumbar Fracture.\",\"authors\":\"Sajid Atique, Ahammed Mekkodathil, Tariq Siddiqui, Saji Mathradikkal, Khalid Ahmed, Mushreq Al-Ani, Ahad Kanbar, Abubaker Alaieb, Suhail Hakim, Basil Younis, Ahmed Ajaj, Aldwin Guerrero, Maarij Masood, Sherwan Khoschnau, Abdel Aziz Hammo, Nuri Abdurraheim, Husham Abdelrahman, Ruben Peralta, Syed Nabir, Shatha Al-Hilli, Ayman El-Menyar, Hassan Al-Thani\",\"doi\":\"10.4103/jets.jets_145_23\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The primary objective of this study was to assess the effectiveness of the clinical decision tool (CDT) in trauma patients, providing a comparable ability to rule out thoracolumbar (TL) fractures as traditional imaging methods. The goal is to facilitate early clearance of the TL spine without an immediate requirement for radiological tests, thereby minimizing unnecessary utilization of TL-spine imaging.</p><p><strong>Methods: </strong>A prospective, observational study was conducted on trauma patients with suspected TL injury. To achieve early TL clearance, the CDT assessed criteria such as absence of pain, tenderness, and pain-free axial movement and flexion. The study enrolled alert trauma patients with thoracic and/or lumbar spine injuries, defined by the Glasgow Coma Scale of 15. The study excluded patients not aligning with CDT criteria, such as those who received intravenous opioid analgesia within 4 h and those unable to stand due to suspected pelvic or lower limb injuries.</p><p><strong>Results: </strong>Following the completion of the CDT steps, there were 31 true negative cases, signifying the absence of TL fractures according to both CDT and imaging studies. The sensitivity of the CDT was 99.38% (95% confidence interval [CI]: 96.59%-99.98%), specificity 9.1% (95% CI: 6.30%-12.73%), negative predictive value (NPV) 96.87% (95% CI: 81.02%-99.56%), positive predictive value (PPV) 34.19% (95% CI: 33.38%-35.00%), negative likelihood ratio (LHR) 0.07 (95% CI: 0.01-0.49), and positive LHR 1.09 (95% CI: 1.06-1.13). The sensitivity, specificity, NPV, PPV, negative LHR, and positive LHR varied with each step in the CDT. Notably, the overall sensitivity was high; however, the stepwise sensitivity decreased, albeit with an improvement in specificity with each further step in the tool. The overall sensitivity in the study cohort (<i>n</i> = 500) was high; however, the stepwise sensitivity decreased, albeit with an improvement in the specificity.</p><p><strong>Conclusions: </strong>The CDT to rule out TL fracture is a feasible bedside stepwise tool in fully awake trauma patients after a thorough clinical neurological examination on arrival. The tool could help Level II or III trauma centers avoid secondary triage to the higher center.</p>\",\"PeriodicalId\":15692,\"journal\":{\"name\":\"Journal of Emergencies, Trauma, and Shock\",\"volume\":\"17 3\",\"pages\":\"159-165\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2024-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11563237/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Emergencies, Trauma, and Shock\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jets.jets_145_23\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Emergencies, Trauma, and Shock","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jets.jets_145_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/2 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Diagnostic Clinical Tool in Trauma Patients to Rule out Thoracolumbar Fracture.
Introduction: The primary objective of this study was to assess the effectiveness of the clinical decision tool (CDT) in trauma patients, providing a comparable ability to rule out thoracolumbar (TL) fractures as traditional imaging methods. The goal is to facilitate early clearance of the TL spine without an immediate requirement for radiological tests, thereby minimizing unnecessary utilization of TL-spine imaging.
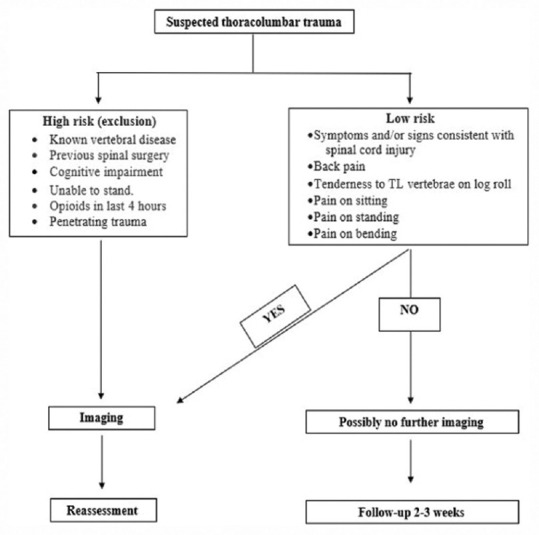
Methods: A prospective, observational study was conducted on trauma patients with suspected TL injury. To achieve early TL clearance, the CDT assessed criteria such as absence of pain, tenderness, and pain-free axial movement and flexion. The study enrolled alert trauma patients with thoracic and/or lumbar spine injuries, defined by the Glasgow Coma Scale of 15. The study excluded patients not aligning with CDT criteria, such as those who received intravenous opioid analgesia within 4 h and those unable to stand due to suspected pelvic or lower limb injuries.
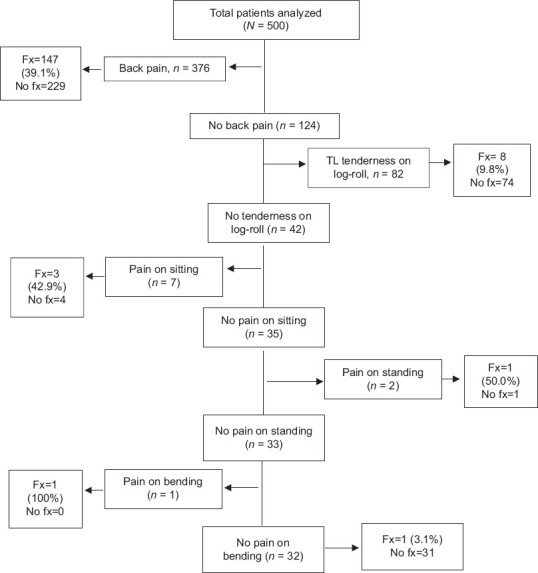
Results: Following the completion of the CDT steps, there were 31 true negative cases, signifying the absence of TL fractures according to both CDT and imaging studies. The sensitivity of the CDT was 99.38% (95% confidence interval [CI]: 96.59%-99.98%), specificity 9.1% (95% CI: 6.30%-12.73%), negative predictive value (NPV) 96.87% (95% CI: 81.02%-99.56%), positive predictive value (PPV) 34.19% (95% CI: 33.38%-35.00%), negative likelihood ratio (LHR) 0.07 (95% CI: 0.01-0.49), and positive LHR 1.09 (95% CI: 1.06-1.13). The sensitivity, specificity, NPV, PPV, negative LHR, and positive LHR varied with each step in the CDT. Notably, the overall sensitivity was high; however, the stepwise sensitivity decreased, albeit with an improvement in specificity with each further step in the tool. The overall sensitivity in the study cohort (n = 500) was high; however, the stepwise sensitivity decreased, albeit with an improvement in the specificity.
Conclusions: The CDT to rule out TL fracture is a feasible bedside stepwise tool in fully awake trauma patients after a thorough clinical neurological examination on arrival. The tool could help Level II or III trauma centers avoid secondary triage to the higher center.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


