Ruixin Zhu, Ran Wang, Jingjing He, Langrun Wang, Huiyu Chen, Xiaokang Niu, You Sun, Yiran Guan, Yifan Gong, Liwei Zhang, Peng An, Keji Li, Fazheng Ren, Weili Xu, Jie Guo
{"title":"按健康的社会决定因素划分的心血管-肾脏-代谢综合征阶段的流行率。","authors":"Ruixin Zhu, Ran Wang, Jingjing He, Langrun Wang, Huiyu Chen, Xiaokang Niu, You Sun, Yiran Guan, Yifan Gong, Liwei Zhang, Peng An, Keji Li, Fazheng Ren, Weili Xu, Jie Guo","doi":"10.1001/jamanetworkopen.2024.45309","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Cardiovascular-kidney-metabolic (CKM) syndrome-a novel, multistage, multisystem disorder as defined by the American Heart Association-is highly prevalent in the US. However, the prevalence of CKM stages by social determinants of health (SDOH) remains unclear.</p><p><strong>Objective: </strong>To investigate whether the prevalence of CKM stages varies by SDOH in US adults.</p><p><strong>Design, setting, and participants: </strong>This cross-sectional study used data from the National Health and Nutrition Examination Survey (1999-2018) and included a nationally representative sample of adults aged 30 to 79 years through complex, multistage probability sampling. Data were analyzed from April 1 to June 15, 2024.</p><p><strong>Exposures: </strong>The exposures included 5 CKM stages (ie, stages 0-4) reflecting progressive pathophysiology, with advanced (stages 3 or 4) and nonadvanced (stages 0, 1, or 2) disease. CKM stages were defined based on risk factors for metabolic syndrome, cardiovascular disease, and chronic kidney disease.</p><p><strong>Main outcome and measures: </strong>The main outcome was the age-standardized prevalence of CKM stages and advanced CKM stages across SDOH, including education, marital status, family income, food security, health insurance, employment, home ownership, and health care access.</p><p><strong>Results: </strong>Among 29 722 participants (weighted mean [SE] age, 50.8 [0.1] years; weighted 50.7% male), the age-standardized prevalence of CKM stages 0 to 4 was 13.6% (95% CI, 13.0%-14.3%), 29.9% (95% CI, 29.1%-30.7%), 43.7% (95% CI, 42.9%-44.5%), 4.7% (95% CI, 4.4%-5.0%), and 8.1% (95% CI, 7.6%-8.5%), respectively. Significant differences were observed in the prevalence of CKM stages across all unfavorable SDOH of interest compared with their favorable counterparts, with unemployment (18.8% [95% CI, 17.7%-20.1%] vs 11.4% [95% CI, 11.0%-11.9%]), low family income (16.1% [95% CI, 15.4%-16.8%] vs 10.1% [95% CI, 9.5%-10.7%]), and food insecurity (18.3% [95% CI, 17.1%-19.6%] vs 11.7% [95% CI, 11.2%-12.2%]) associated with an increased likelihood of advanced CKM stages. Participants with 2 or more unfavorable SDOH were more likely to have advanced CKM stages (age-standardized prevalence, 15.8% [95% CI, 15.2%-16.5%] vs 10.5% [95% CI, 9.9%-11.1%] with <2 unfavorable SDOH). Living in a rented home (15.9% [95% CI, 14.7%-17.0%] vs 9.3% [95% CI, 8.7%-9.9%] owning the home) or not living with a partner (13.2% [95% CI, 12.3%-14.3%] vs 9.2% [95% CI, 8.5%-9.8%] living with a partner) increased the likelihood of advanced CKM stages in female but not male participants.</p><p><strong>Conclusions and relevance: </strong>In this cross-sectional study, disparities in the prevalence of CKM stages by SDOH, particularly family income, food security, and employment, with notable sex differences, were observed in US adults. These findings highlight the need to address inequities in CKM syndrome through targeted interventions.</p>","PeriodicalId":14694,"journal":{"name":"JAMA Network Open","volume":"7 11","pages":"e2445309"},"PeriodicalIF":9.7000,"publicationDate":"2024-11-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11574692/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prevalence of Cardiovascular-Kidney-Metabolic Syndrome Stages by Social Determinants of Health.\",\"authors\":\"Ruixin Zhu, Ran Wang, Jingjing He, Langrun Wang, Huiyu Chen, Xiaokang Niu, You Sun, Yiran Guan, Yifan Gong, Liwei Zhang, Peng An, Keji Li, Fazheng Ren, Weili Xu, Jie Guo\",\"doi\":\"10.1001/jamanetworkopen.2024.45309\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>Cardiovascular-kidney-metabolic (CKM) syndrome-a novel, multistage, multisystem disorder as defined by the American Heart Association-is highly prevalent in the US. However, the prevalence of CKM stages by social determinants of health (SDOH) remains unclear.</p><p><strong>Objective: </strong>To investigate whether the prevalence of CKM stages varies by SDOH in US adults.</p><p><strong>Design, setting, and participants: </strong>This cross-sectional study used data from the National Health and Nutrition Examination Survey (1999-2018) and included a nationally representative sample of adults aged 30 to 79 years through complex, multistage probability sampling. Data were analyzed from April 1 to June 15, 2024.</p><p><strong>Exposures: </strong>The exposures included 5 CKM stages (ie, stages 0-4) reflecting progressive pathophysiology, with advanced (stages 3 or 4) and nonadvanced (stages 0, 1, or 2) disease. CKM stages were defined based on risk factors for metabolic syndrome, cardiovascular disease, and chronic kidney disease.</p><p><strong>Main outcome and measures: </strong>The main outcome was the age-standardized prevalence of CKM stages and advanced CKM stages across SDOH, including education, marital status, family income, food security, health insurance, employment, home ownership, and health care access.</p><p><strong>Results: </strong>Among 29 722 participants (weighted mean [SE] age, 50.8 [0.1] years; weighted 50.7% male), the age-standardized prevalence of CKM stages 0 to 4 was 13.6% (95% CI, 13.0%-14.3%), 29.9% (95% CI, 29.1%-30.7%), 43.7% (95% CI, 42.9%-44.5%), 4.7% (95% CI, 4.4%-5.0%), and 8.1% (95% CI, 7.6%-8.5%), respectively. Significant differences were observed in the prevalence of CKM stages across all unfavorable SDOH of interest compared with their favorable counterparts, with unemployment (18.8% [95% CI, 17.7%-20.1%] vs 11.4% [95% CI, 11.0%-11.9%]), low family income (16.1% [95% CI, 15.4%-16.8%] vs 10.1% [95% CI, 9.5%-10.7%]), and food insecurity (18.3% [95% CI, 17.1%-19.6%] vs 11.7% [95% CI, 11.2%-12.2%]) associated with an increased likelihood of advanced CKM stages. Participants with 2 or more unfavorable SDOH were more likely to have advanced CKM stages (age-standardized prevalence, 15.8% [95% CI, 15.2%-16.5%] vs 10.5% [95% CI, 9.9%-11.1%] with <2 unfavorable SDOH). Living in a rented home (15.9% [95% CI, 14.7%-17.0%] vs 9.3% [95% CI, 8.7%-9.9%] owning the home) or not living with a partner (13.2% [95% CI, 12.3%-14.3%] vs 9.2% [95% CI, 8.5%-9.8%] living with a partner) increased the likelihood of advanced CKM stages in female but not male participants.</p><p><strong>Conclusions and relevance: </strong>In this cross-sectional study, disparities in the prevalence of CKM stages by SDOH, particularly family income, food security, and employment, with notable sex differences, were observed in US adults. These findings highlight the need to address inequities in CKM syndrome through targeted interventions.</p>\",\"PeriodicalId\":14694,\"journal\":{\"name\":\"JAMA Network Open\",\"volume\":\"7 11\",\"pages\":\"e2445309\"},\"PeriodicalIF\":9.7000,\"publicationDate\":\"2024-11-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11574692/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMA Network Open\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1001/jamanetworkopen.2024.45309\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Network Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1001/jamanetworkopen.2024.45309","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Prevalence of Cardiovascular-Kidney-Metabolic Syndrome Stages by Social Determinants of Health.
Importance: Cardiovascular-kidney-metabolic (CKM) syndrome-a novel, multistage, multisystem disorder as defined by the American Heart Association-is highly prevalent in the US. However, the prevalence of CKM stages by social determinants of health (SDOH) remains unclear.
Objective: To investigate whether the prevalence of CKM stages varies by SDOH in US adults.
Design, setting, and participants: This cross-sectional study used data from the National Health and Nutrition Examination Survey (1999-2018) and included a nationally representative sample of adults aged 30 to 79 years through complex, multistage probability sampling. Data were analyzed from April 1 to June 15, 2024.
Exposures: The exposures included 5 CKM stages (ie, stages 0-4) reflecting progressive pathophysiology, with advanced (stages 3 or 4) and nonadvanced (stages 0, 1, or 2) disease. CKM stages were defined based on risk factors for metabolic syndrome, cardiovascular disease, and chronic kidney disease.
Main outcome and measures: The main outcome was the age-standardized prevalence of CKM stages and advanced CKM stages across SDOH, including education, marital status, family income, food security, health insurance, employment, home ownership, and health care access.
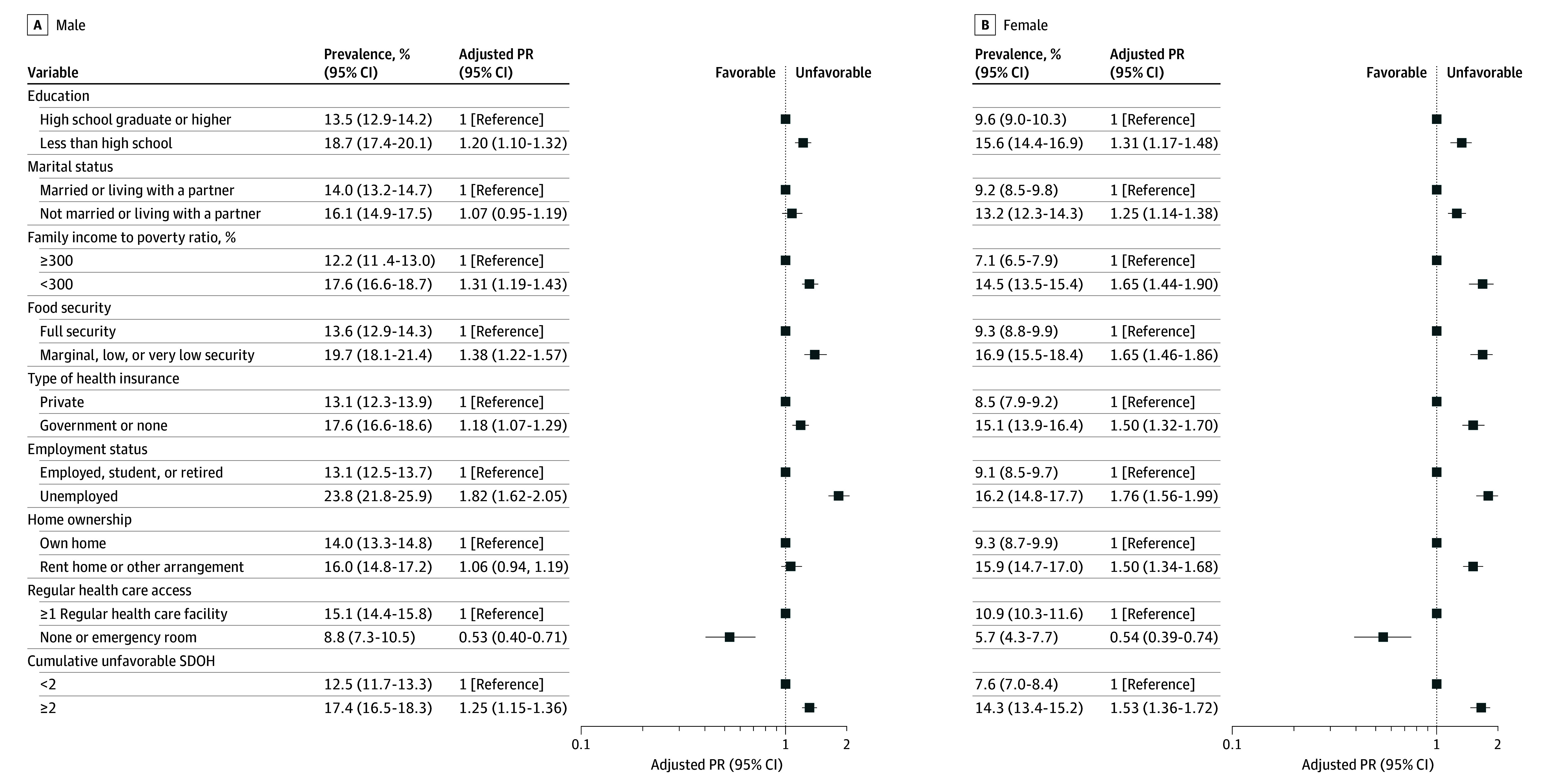
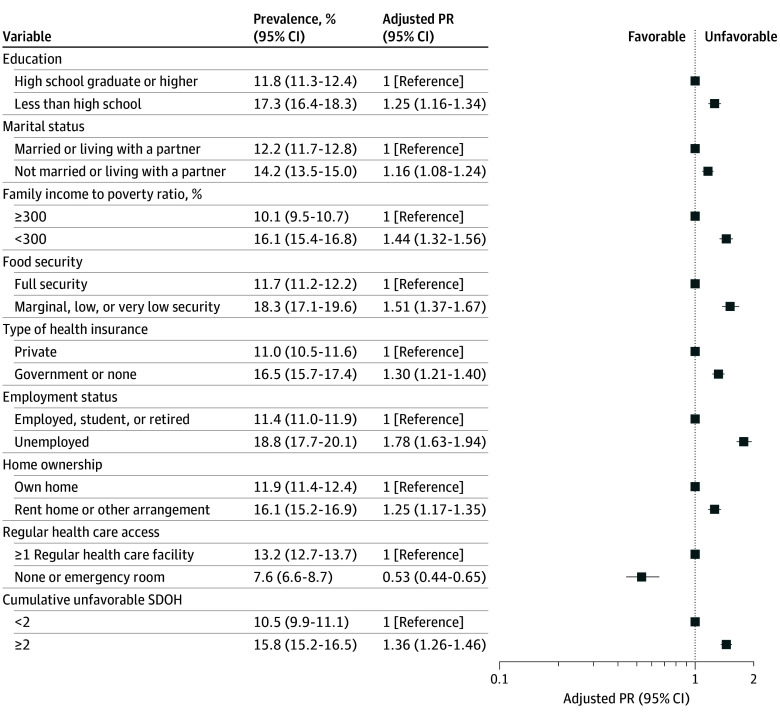
Results: Among 29 722 participants (weighted mean [SE] age, 50.8 [0.1] years; weighted 50.7% male), the age-standardized prevalence of CKM stages 0 to 4 was 13.6% (95% CI, 13.0%-14.3%), 29.9% (95% CI, 29.1%-30.7%), 43.7% (95% CI, 42.9%-44.5%), 4.7% (95% CI, 4.4%-5.0%), and 8.1% (95% CI, 7.6%-8.5%), respectively. Significant differences were observed in the prevalence of CKM stages across all unfavorable SDOH of interest compared with their favorable counterparts, with unemployment (18.8% [95% CI, 17.7%-20.1%] vs 11.4% [95% CI, 11.0%-11.9%]), low family income (16.1% [95% CI, 15.4%-16.8%] vs 10.1% [95% CI, 9.5%-10.7%]), and food insecurity (18.3% [95% CI, 17.1%-19.6%] vs 11.7% [95% CI, 11.2%-12.2%]) associated with an increased likelihood of advanced CKM stages. Participants with 2 or more unfavorable SDOH were more likely to have advanced CKM stages (age-standardized prevalence, 15.8% [95% CI, 15.2%-16.5%] vs 10.5% [95% CI, 9.9%-11.1%] with <2 unfavorable SDOH). Living in a rented home (15.9% [95% CI, 14.7%-17.0%] vs 9.3% [95% CI, 8.7%-9.9%] owning the home) or not living with a partner (13.2% [95% CI, 12.3%-14.3%] vs 9.2% [95% CI, 8.5%-9.8%] living with a partner) increased the likelihood of advanced CKM stages in female but not male participants.
Conclusions and relevance: In this cross-sectional study, disparities in the prevalence of CKM stages by SDOH, particularly family income, food security, and employment, with notable sex differences, were observed in US adults. These findings highlight the need to address inequities in CKM syndrome through targeted interventions.
期刊介绍:
JAMA Network Open, a member of the esteemed JAMA Network, stands as an international, peer-reviewed, open-access general medical journal.The publication is dedicated to disseminating research across various health disciplines and countries, encompassing clinical care, innovation in health care, health policy, and global health.
JAMA Network Open caters to clinicians, investigators, and policymakers, providing a platform for valuable insights and advancements in the medical field. As part of the JAMA Network, a consortium of peer-reviewed general medical and specialty publications, JAMA Network Open contributes to the collective knowledge and understanding within the medical community.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


