{"title":"染色体高度不稳定与激素受体阳性、人表皮生长因子受体 2 阴性乳腺癌患者 10 年复发风险较高有关:一项大规模、多地点、回顾性研究的临床证据。","authors":"Yu-Yang Liao, Jianfei Fu, Xiang Lu, Ziliang Qian, Yang Yu, Liang Zhu, Jia-Ni Pan, Pu-Chun Li, Qiao-Yan Zhu, Xiaolin Li, Wenyong Sun, Xiao-Jia Wang, Wen-Ming Cao","doi":"10.1002/2056-4538.70011","DOIUrl":null,"url":null,"abstract":"<p>Long-term survival varies among hormone receptor-positive (HR+) and human epidermal growth factor receptor 2-negative (HER2−) breast cancer patients and is seriously impaired by metastasis. Chromosomal instability (CIN) was one of the key drivers of breast cancer metastasis. Here we evaluate CIN and 10-year invasive disease-free survival (iDFS) and overall survival (OS) in HR+/HER2−– breast cancer. In this large-scale, multiple-site, retrospective study, 354 HR+/HER2− breast cancer patients were recruited. Of these, 204 patients were used for internal training, 70 for external validation, and 80 for cross-validation. All medical records were carefully reviewed to obtain the disease recurrence information. Formalin-fixed paraffin-embedded tissue samples were collected, followed by low-pass whole-genome sequencing with a median genome coverage of 1.86X using minimal 1 ng DNA input. CIN was then assessed using a customized bioinformatics workflow. Three or more instances of CIN per sample was defined as high CIN and the frequency was 42.2% (86/204) in the internal cohort. High CIN correlated significantly with increased lymph node metastasis, vascular invasion, progesterone receptor negative status, HER2 low, worse pathological type, and performed as an independent prognostic factor for HR+/− breast cancer. Patients with high CIN had shorter iDFS and OS than those with low CIN [10-year iDFS 11.1% versus 82.2%, hazard ratio (HR) = 11.12, <i>p</i> < 0.01; 10-year OS 45.7% versus 94.3%, HR = 14.17, <i>p</i> < 0.01]. These findings were validated in two external cohorts with 70 breast cancer patients. Moreover, high CIN could predict the prognosis more accurately than Adjuvant! Online score (10-year iDFS 11.1% versus 48.6%, HR = 2.71, <i>p</i> < 0.01). Cross-validation analysis found that high consistency (83.8%) was observed between CIN and MammaPrint score, while only 45% between CIN and Adjuvant! Online score. In conclusion, high CIN is an independent prognostic indicator for HR+/HER2− breast cancer with shorter iDFS and OS and holds promise for predicting recurrence and metastasis.</p>","PeriodicalId":48612,"journal":{"name":"Journal of Pathology Clinical Research","volume":"10 6","pages":""},"PeriodicalIF":3.7000,"publicationDate":"2024-11-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/2056-4538.70011","citationCount":"0","resultStr":"{\"title\":\"High chromosomal instability is associated with higher 10-year risks of recurrence for hormone receptor-positive, human epidermal growth factor receptor 2-negative breast cancer patients: clinical evidence from a large-scale, multiple-site, retrospective study\",\"authors\":\"Yu-Yang Liao, Jianfei Fu, Xiang Lu, Ziliang Qian, Yang Yu, Liang Zhu, Jia-Ni Pan, Pu-Chun Li, Qiao-Yan Zhu, Xiaolin Li, Wenyong Sun, Xiao-Jia Wang, Wen-Ming Cao\",\"doi\":\"10.1002/2056-4538.70011\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Long-term survival varies among hormone receptor-positive (HR+) and human epidermal growth factor receptor 2-negative (HER2−) breast cancer patients and is seriously impaired by metastasis. Chromosomal instability (CIN) was one of the key drivers of breast cancer metastasis. Here we evaluate CIN and 10-year invasive disease-free survival (iDFS) and overall survival (OS) in HR+/HER2−– breast cancer. In this large-scale, multiple-site, retrospective study, 354 HR+/HER2− breast cancer patients were recruited. Of these, 204 patients were used for internal training, 70 for external validation, and 80 for cross-validation. All medical records were carefully reviewed to obtain the disease recurrence information. Formalin-fixed paraffin-embedded tissue samples were collected, followed by low-pass whole-genome sequencing with a median genome coverage of 1.86X using minimal 1 ng DNA input. CIN was then assessed using a customized bioinformatics workflow. Three or more instances of CIN per sample was defined as high CIN and the frequency was 42.2% (86/204) in the internal cohort. High CIN correlated significantly with increased lymph node metastasis, vascular invasion, progesterone receptor negative status, HER2 low, worse pathological type, and performed as an independent prognostic factor for HR+/− breast cancer. Patients with high CIN had shorter iDFS and OS than those with low CIN [10-year iDFS 11.1% versus 82.2%, hazard ratio (HR) = 11.12, <i>p</i> < 0.01; 10-year OS 45.7% versus 94.3%, HR = 14.17, <i>p</i> < 0.01]. These findings were validated in two external cohorts with 70 breast cancer patients. Moreover, high CIN could predict the prognosis more accurately than Adjuvant! Online score (10-year iDFS 11.1% versus 48.6%, HR = 2.71, <i>p</i> < 0.01). Cross-validation analysis found that high consistency (83.8%) was observed between CIN and MammaPrint score, while only 45% between CIN and Adjuvant! Online score. In conclusion, high CIN is an independent prognostic indicator for HR+/HER2− breast cancer with shorter iDFS and OS and holds promise for predicting recurrence and metastasis.</p>\",\"PeriodicalId\":48612,\"journal\":{\"name\":\"Journal of Pathology Clinical Research\",\"volume\":\"10 6\",\"pages\":\"\"},\"PeriodicalIF\":3.7000,\"publicationDate\":\"2024-11-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/2056-4538.70011\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Pathology Clinical Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/2056-4538.70011\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PATHOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pathology Clinical Research","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/2056-4538.70011","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PATHOLOGY","Score":null,"Total":0}
High chromosomal instability is associated with higher 10-year risks of recurrence for hormone receptor-positive, human epidermal growth factor receptor 2-negative breast cancer patients: clinical evidence from a large-scale, multiple-site, retrospective study
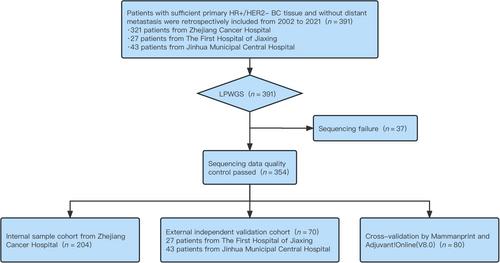
Long-term survival varies among hormone receptor-positive (HR+) and human epidermal growth factor receptor 2-negative (HER2−) breast cancer patients and is seriously impaired by metastasis. Chromosomal instability (CIN) was one of the key drivers of breast cancer metastasis. Here we evaluate CIN and 10-year invasive disease-free survival (iDFS) and overall survival (OS) in HR+/HER2−– breast cancer. In this large-scale, multiple-site, retrospective study, 354 HR+/HER2− breast cancer patients were recruited. Of these, 204 patients were used for internal training, 70 for external validation, and 80 for cross-validation. All medical records were carefully reviewed to obtain the disease recurrence information. Formalin-fixed paraffin-embedded tissue samples were collected, followed by low-pass whole-genome sequencing with a median genome coverage of 1.86X using minimal 1 ng DNA input. CIN was then assessed using a customized bioinformatics workflow. Three or more instances of CIN per sample was defined as high CIN and the frequency was 42.2% (86/204) in the internal cohort. High CIN correlated significantly with increased lymph node metastasis, vascular invasion, progesterone receptor negative status, HER2 low, worse pathological type, and performed as an independent prognostic factor for HR+/− breast cancer. Patients with high CIN had shorter iDFS and OS than those with low CIN [10-year iDFS 11.1% versus 82.2%, hazard ratio (HR) = 11.12, p < 0.01; 10-year OS 45.7% versus 94.3%, HR = 14.17, p < 0.01]. These findings were validated in two external cohorts with 70 breast cancer patients. Moreover, high CIN could predict the prognosis more accurately than Adjuvant! Online score (10-year iDFS 11.1% versus 48.6%, HR = 2.71, p < 0.01). Cross-validation analysis found that high consistency (83.8%) was observed between CIN and MammaPrint score, while only 45% between CIN and Adjuvant! Online score. In conclusion, high CIN is an independent prognostic indicator for HR+/HER2− breast cancer with shorter iDFS and OS and holds promise for predicting recurrence and metastasis.
期刊介绍:
The Journal of Pathology: Clinical Research and The Journal of Pathology serve as translational bridges between basic biomedical science and clinical medicine with particular emphasis on, but not restricted to, tissue based studies.
The focus of The Journal of Pathology: Clinical Research is the publication of studies that illuminate the clinical relevance of research in the broad area of the study of disease. Appropriately powered and validated studies with novel diagnostic, prognostic and predictive significance, and biomarker discover and validation, will be welcomed. Studies with a predominantly mechanistic basis will be more appropriate for the companion Journal of Pathology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


