{"title":"以色列人群中林奇综合征的遗传情况。","authors":"Aasem Abu Shtaya, Sofia Naftaly Nathan, Inbal Kedar, Eitan Friedman, Elizabeth Half, Gabi Lidzbarsky, Gili Reznick Levi, Ido Laish, Lior Katz, Lily Bazak, Lilach Peled Peretz, Lina Basel Salmon, Liza Douiev, Marina Lifshitc Kalis, Menachem Schechter, Michal Barzily-Rokni, Nadra Nasser Samra, Naim Abu-Freha, Ofir Hagari-Bechar, Ori Segol, Samar Mattar, Sarit Farage Barhom, Shikma Mordechai, Shiri Shkedi Rafid, Stavit A Shalev, Tamar Peretz-Yablonski, Zohar Levi, Revital Bruchim, Chana Vinkler, Rinat Bernstein-Molho, Sari Lieberman, Yael Goldberg","doi":"10.1007/s10689-024-00432-w","DOIUrl":null,"url":null,"abstract":"<p><p>Deciphering the spectrum and founder disease-causing variants (DCVs) in specific populations can shape and facilitate the diagnostic process of Lynch Syndrome (LS). The aim of this report was to comprehensively update on the genetic landscape of LS in the ethnically diverse Israeli-Jewish population. The cohort included 1080 carriers from 588 families; some from underrepresented, understudied Israeli ethnic groups recruited from 8 genetic institutes and high-risk clinics throughout the country. Variant classification was performed according to the American College of Medical Genetics criteria. A total of 157 DCVs were identified, 12 are reported here for the first time, and 9 reclassified. MSH2 DCVs were identified in 286 families (49%). Most DCVs (125/157, 80%) were noted in one or two families only. Sixteen DCVs, each detected in ≥ 5 families, and accounted for LS in 378/588 (64%) families. Constitutional mismatch repair deficiency (CMMRD) was diagnosed in 7 families. Twenty-five carriers (2.3%) had an additional DCV or risk alleles in another cancer susceptibility gene. In conclusion, MMR gene variant distribution in Israel is diverse. MSH2 is most commonly mutated due to founder DCVs. Though the 16 prevalent LS-associated DCVs were frequently detected in our cohort, none of them is frequently reported in the general population. These data should facilitate variant interpretation, spouse and cascade testing.</p>","PeriodicalId":12336,"journal":{"name":"Familial Cancer","volume":"24 1","pages":"6"},"PeriodicalIF":2.0000,"publicationDate":"2024-11-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11567984/pdf/","citationCount":"0","resultStr":"{\"title\":\"The genetic landscape of Lynch syndrome in the Israeli population.\",\"authors\":\"Aasem Abu Shtaya, Sofia Naftaly Nathan, Inbal Kedar, Eitan Friedman, Elizabeth Half, Gabi Lidzbarsky, Gili Reznick Levi, Ido Laish, Lior Katz, Lily Bazak, Lilach Peled Peretz, Lina Basel Salmon, Liza Douiev, Marina Lifshitc Kalis, Menachem Schechter, Michal Barzily-Rokni, Nadra Nasser Samra, Naim Abu-Freha, Ofir Hagari-Bechar, Ori Segol, Samar Mattar, Sarit Farage Barhom, Shikma Mordechai, Shiri Shkedi Rafid, Stavit A Shalev, Tamar Peretz-Yablonski, Zohar Levi, Revital Bruchim, Chana Vinkler, Rinat Bernstein-Molho, Sari Lieberman, Yael Goldberg\",\"doi\":\"10.1007/s10689-024-00432-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Deciphering the spectrum and founder disease-causing variants (DCVs) in specific populations can shape and facilitate the diagnostic process of Lynch Syndrome (LS). The aim of this report was to comprehensively update on the genetic landscape of LS in the ethnically diverse Israeli-Jewish population. The cohort included 1080 carriers from 588 families; some from underrepresented, understudied Israeli ethnic groups recruited from 8 genetic institutes and high-risk clinics throughout the country. Variant classification was performed according to the American College of Medical Genetics criteria. A total of 157 DCVs were identified, 12 are reported here for the first time, and 9 reclassified. MSH2 DCVs were identified in 286 families (49%). Most DCVs (125/157, 80%) were noted in one or two families only. Sixteen DCVs, each detected in ≥ 5 families, and accounted for LS in 378/588 (64%) families. Constitutional mismatch repair deficiency (CMMRD) was diagnosed in 7 families. Twenty-five carriers (2.3%) had an additional DCV or risk alleles in another cancer susceptibility gene. In conclusion, MMR gene variant distribution in Israel is diverse. MSH2 is most commonly mutated due to founder DCVs. Though the 16 prevalent LS-associated DCVs were frequently detected in our cohort, none of them is frequently reported in the general population. These data should facilitate variant interpretation, spouse and cascade testing.</p>\",\"PeriodicalId\":12336,\"journal\":{\"name\":\"Familial Cancer\",\"volume\":\"24 1\",\"pages\":\"6\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-11-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11567984/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Familial Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10689-024-00432-w\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GENETICS & HEREDITY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Familial Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10689-024-00432-w","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
The genetic landscape of Lynch syndrome in the Israeli population.
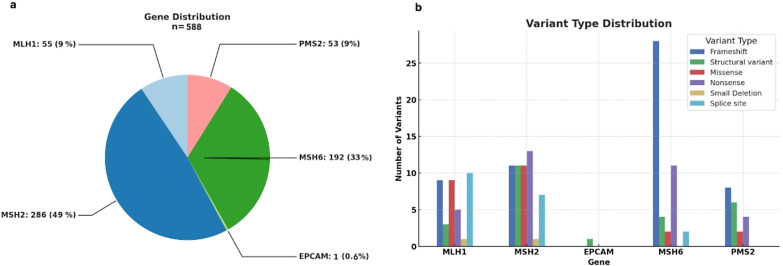
Deciphering the spectrum and founder disease-causing variants (DCVs) in specific populations can shape and facilitate the diagnostic process of Lynch Syndrome (LS). The aim of this report was to comprehensively update on the genetic landscape of LS in the ethnically diverse Israeli-Jewish population. The cohort included 1080 carriers from 588 families; some from underrepresented, understudied Israeli ethnic groups recruited from 8 genetic institutes and high-risk clinics throughout the country. Variant classification was performed according to the American College of Medical Genetics criteria. A total of 157 DCVs were identified, 12 are reported here for the first time, and 9 reclassified. MSH2 DCVs were identified in 286 families (49%). Most DCVs (125/157, 80%) were noted in one or two families only. Sixteen DCVs, each detected in ≥ 5 families, and accounted for LS in 378/588 (64%) families. Constitutional mismatch repair deficiency (CMMRD) was diagnosed in 7 families. Twenty-five carriers (2.3%) had an additional DCV or risk alleles in another cancer susceptibility gene. In conclusion, MMR gene variant distribution in Israel is diverse. MSH2 is most commonly mutated due to founder DCVs. Though the 16 prevalent LS-associated DCVs were frequently detected in our cohort, none of them is frequently reported in the general population. These data should facilitate variant interpretation, spouse and cascade testing.
期刊介绍:
In recent years clinical cancer genetics has become increasingly important. Several events, in particular the developments in DNA-based technology, have contributed to this evolution. Clinical cancer genetics has now matured to a medical discipline which is truly multidisciplinary in which clinical and molecular geneticists work together with clinical and medical oncologists as well as with psycho-social workers.
Due to the multidisciplinary nature of clinical cancer genetics most papers are currently being published in a wide variety of journals on epidemiology, oncology and genetics. Familial Cancer provides a forum bringing these topics together focusing on the interests and needs of the clinician.
The journal mainly concentrates on clinical cancer genetics. Most major areas in the field shall be included, such as epidemiology of familial cancer, molecular analysis and diagnosis, clinical expression, treatment and prevention, counselling and the health economics of familial cancer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


