Christina Ekenbäck, Jonas Persson, Per Tornvall, Lena Forsberg, Jonas Spaak
{"title":"交感神经活动和塔克次博综合征对生理压力的反应。","authors":"Christina Ekenbäck, Jonas Persson, Per Tornvall, Lena Forsberg, Jonas Spaak","doi":"10.1007/s10286-024-01082-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The prevailing hypothesis posits that Takotsubo syndrome (TTS) is caused by massive sympathetic activation, yet supporting evidence remains inconsistent. The objectives of the present study were to determine whether sympathetic activity and reactivity are enhanced in the recovery phase of TTS, and to evaluate the effect of selective β1-receptor blockade on sympathetic reactivity.</p><p><strong>Methods: </strong>We conducted a case-control study that included 18 female patients with TTS and 13 age- and sex-matched controls. Muscle sympathetic nerve activity was measured through microneurography of the peroneal nerve at rest and during the cold pressor test. In the TTS group, recordings were repeated after randomisation to intravenous metoprolol or placebo. In 10 TTS patients, cardiac sympathetic activity was assessed using iodine 123-metaiodobenzylguanidine scintigraphy. Blood samples were collected during hospitalisation.</p><p><strong>Results: </strong>Microneurography was performed a median of 27.5 days after patient admission. There were no significant differences in burst incidence, burst frequency, burst height or burst area between the TTS patients and the controls at rest, during stress or after administration of intravenous metoprolol. Iodine 123-metaiodobenzylguanidine scintigraphy was performed a median of 12.5 days after admission, revealing decreased early 1.54 ± 0.13 and late 1.40 ± 0.13 heart-to-mediastinum ratios, and an increased washout rate of 41.8 ± 12.1%. Catecholamine metabolites were comparable between the study groups.</p><p><strong>Conclusion: </strong>General sympathetic hyperactivity or hyperreactivity unlikely contributes to TTS, as catecholamine levels and muscle sympathetic nerve activity at rest and during stress were similar between the TTS patients and the controls. As scintigraphy showed increased cardiac sympathetic activity, a pathological cardiac adrenergic response and vulnerability to sympathetic activation may be crucial for the development of the syndrome.</p>","PeriodicalId":10168,"journal":{"name":"Clinical Autonomic Research","volume":" ","pages":"205-214"},"PeriodicalIF":3.4000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12000160/pdf/","citationCount":"0","resultStr":"{\"title\":\"Sympathetic nerve activity and response to physiological stress in Takotsubo syndrome.\",\"authors\":\"Christina Ekenbäck, Jonas Persson, Per Tornvall, Lena Forsberg, Jonas Spaak\",\"doi\":\"10.1007/s10286-024-01082-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>The prevailing hypothesis posits that Takotsubo syndrome (TTS) is caused by massive sympathetic activation, yet supporting evidence remains inconsistent. The objectives of the present study were to determine whether sympathetic activity and reactivity are enhanced in the recovery phase of TTS, and to evaluate the effect of selective β1-receptor blockade on sympathetic reactivity.</p><p><strong>Methods: </strong>We conducted a case-control study that included 18 female patients with TTS and 13 age- and sex-matched controls. Muscle sympathetic nerve activity was measured through microneurography of the peroneal nerve at rest and during the cold pressor test. In the TTS group, recordings were repeated after randomisation to intravenous metoprolol or placebo. In 10 TTS patients, cardiac sympathetic activity was assessed using iodine 123-metaiodobenzylguanidine scintigraphy. Blood samples were collected during hospitalisation.</p><p><strong>Results: </strong>Microneurography was performed a median of 27.5 days after patient admission. There were no significant differences in burst incidence, burst frequency, burst height or burst area between the TTS patients and the controls at rest, during stress or after administration of intravenous metoprolol. Iodine 123-metaiodobenzylguanidine scintigraphy was performed a median of 12.5 days after admission, revealing decreased early 1.54 ± 0.13 and late 1.40 ± 0.13 heart-to-mediastinum ratios, and an increased washout rate of 41.8 ± 12.1%. Catecholamine metabolites were comparable between the study groups.</p><p><strong>Conclusion: </strong>General sympathetic hyperactivity or hyperreactivity unlikely contributes to TTS, as catecholamine levels and muscle sympathetic nerve activity at rest and during stress were similar between the TTS patients and the controls. As scintigraphy showed increased cardiac sympathetic activity, a pathological cardiac adrenergic response and vulnerability to sympathetic activation may be crucial for the development of the syndrome.</p>\",\"PeriodicalId\":10168,\"journal\":{\"name\":\"Clinical Autonomic Research\",\"volume\":\" \",\"pages\":\"205-214\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12000160/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Autonomic Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10286-024-01082-9\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Autonomic Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10286-024-01082-9","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/15 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Sympathetic nerve activity and response to physiological stress in Takotsubo syndrome.
Purpose: The prevailing hypothesis posits that Takotsubo syndrome (TTS) is caused by massive sympathetic activation, yet supporting evidence remains inconsistent. The objectives of the present study were to determine whether sympathetic activity and reactivity are enhanced in the recovery phase of TTS, and to evaluate the effect of selective β1-receptor blockade on sympathetic reactivity.
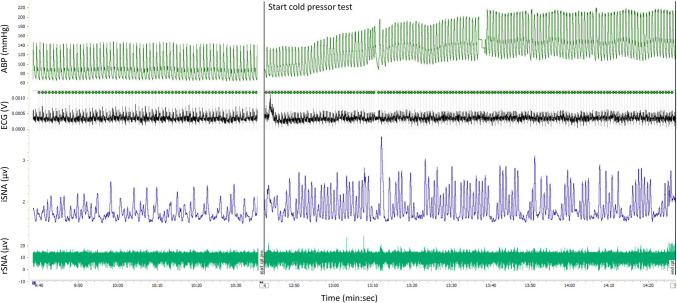
Methods: We conducted a case-control study that included 18 female patients with TTS and 13 age- and sex-matched controls. Muscle sympathetic nerve activity was measured through microneurography of the peroneal nerve at rest and during the cold pressor test. In the TTS group, recordings were repeated after randomisation to intravenous metoprolol or placebo. In 10 TTS patients, cardiac sympathetic activity was assessed using iodine 123-metaiodobenzylguanidine scintigraphy. Blood samples were collected during hospitalisation.
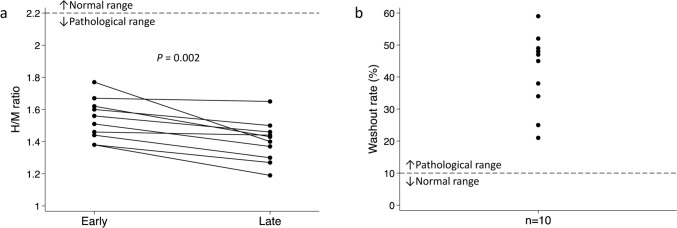
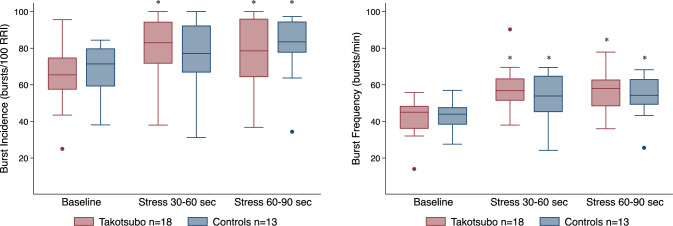
Results: Microneurography was performed a median of 27.5 days after patient admission. There were no significant differences in burst incidence, burst frequency, burst height or burst area between the TTS patients and the controls at rest, during stress or after administration of intravenous metoprolol. Iodine 123-metaiodobenzylguanidine scintigraphy was performed a median of 12.5 days after admission, revealing decreased early 1.54 ± 0.13 and late 1.40 ± 0.13 heart-to-mediastinum ratios, and an increased washout rate of 41.8 ± 12.1%. Catecholamine metabolites were comparable between the study groups.
Conclusion: General sympathetic hyperactivity or hyperreactivity unlikely contributes to TTS, as catecholamine levels and muscle sympathetic nerve activity at rest and during stress were similar between the TTS patients and the controls. As scintigraphy showed increased cardiac sympathetic activity, a pathological cardiac adrenergic response and vulnerability to sympathetic activation may be crucial for the development of the syndrome.
期刊介绍:
Clinical Autonomic Research aims to draw together and disseminate research work from various disciplines and specialties dealing with clinical problems resulting from autonomic dysfunction. Areas to be covered include: cardiovascular system, neurology, diabetes, endocrinology, urology, pain disorders, ophthalmology, gastroenterology, toxicology and clinical pharmacology, skin infectious diseases, renal disease.
This journal is an essential source of new information for everyone working in areas involving the autonomic nervous system. A major feature of Clinical Autonomic Research is its speed of publication coupled with the highest refereeing standards.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


