{"title":"在原发性醛固酮增多症的矿物皮质激素受体拮抗剂治疗中加入萨库比特利/缬沙坦:对血浆醛固酮浓度和血浆肾素活性的影响","authors":"Keisuke Okamura, Masatoshi Matsushima, Yosuke Takamiya, Tetsu Okuda, Hideto Sako, Akihiro Udo, Kenichiro Taniguchi, Shogo Morisaki, Ichiro Imamura, Hidenori Urata, Shin-Ichiro Miura","doi":"10.14740/jocmr6058","DOIUrl":null,"url":null,"abstract":"<p><p>In the pharmacologic treatment of primary aldosteronism (PA), titration of mineralocorticoid receptor antagonist (MRA) dosing is necessary to reverse the renin suppression caused by high aldosterone levels. However, we often encounter cases in which the plasma renin activity (PRA) does not achieve the target level, even with the maximum dose of MRA. In this setting, sacubitril/valsartan, a combination of a neprilysin inhibitor and an angiotensin II type 1 receptor blocker that is approved for use as adjunctive therapy with an MRA, has been reported to inhibit aldosterone secretion both <i>in vitro</i> and <i>in vivo</i>. If sacubitril/valsartan proves to be effective in this context, it may offer a promising treatment for PA. However, there are few reports on the use of sacubitril/valsartan in this disease. We used add-on sacubitril/valsartan in three patients with PA, in whom blood pressure was insufficiently reduced and PRA remained suppressed despite administering the maximum dose of MRA. With the addition of sacubitril/valsartan, the decrease in plasma aldosterone concentration (PAC) was more marked than the increase in PRA. Because MRAs do not suppress aldosterone production but instead act by blocking mineralocorticoid receptors, use of these agents actually promotes the renin-angiotensin system and leads to increased PAC resulting from positive feedback. The pathological significance of the phenomenon whereby PAC increases with MRA administration but decreases with the addition of sacubitril/valsartan is unclear. In PA, more effective treatment may be possible by suppressing aldosterone with sacubitril/valsartan and blocking the action of aldosterone with MRAs.</p>","PeriodicalId":94329,"journal":{"name":"Journal of clinical medicine research","volume":"16 10","pages":"509-517"},"PeriodicalIF":2.0000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11557503/pdf/","citationCount":"0","resultStr":"{\"title\":\"Addition of Sacubitril/Valsartan to Mineralocorticoid Receptor Antagonist Therapy in Primary Aldosteronism: Effects on Plasma Aldosterone Concentration and Plasma Renin Activity.\",\"authors\":\"Keisuke Okamura, Masatoshi Matsushima, Yosuke Takamiya, Tetsu Okuda, Hideto Sako, Akihiro Udo, Kenichiro Taniguchi, Shogo Morisaki, Ichiro Imamura, Hidenori Urata, Shin-Ichiro Miura\",\"doi\":\"10.14740/jocmr6058\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>In the pharmacologic treatment of primary aldosteronism (PA), titration of mineralocorticoid receptor antagonist (MRA) dosing is necessary to reverse the renin suppression caused by high aldosterone levels. However, we often encounter cases in which the plasma renin activity (PRA) does not achieve the target level, even with the maximum dose of MRA. In this setting, sacubitril/valsartan, a combination of a neprilysin inhibitor and an angiotensin II type 1 receptor blocker that is approved for use as adjunctive therapy with an MRA, has been reported to inhibit aldosterone secretion both <i>in vitro</i> and <i>in vivo</i>. If sacubitril/valsartan proves to be effective in this context, it may offer a promising treatment for PA. However, there are few reports on the use of sacubitril/valsartan in this disease. We used add-on sacubitril/valsartan in three patients with PA, in whom blood pressure was insufficiently reduced and PRA remained suppressed despite administering the maximum dose of MRA. With the addition of sacubitril/valsartan, the decrease in plasma aldosterone concentration (PAC) was more marked than the increase in PRA. Because MRAs do not suppress aldosterone production but instead act by blocking mineralocorticoid receptors, use of these agents actually promotes the renin-angiotensin system and leads to increased PAC resulting from positive feedback. The pathological significance of the phenomenon whereby PAC increases with MRA administration but decreases with the addition of sacubitril/valsartan is unclear. In PA, more effective treatment may be possible by suppressing aldosterone with sacubitril/valsartan and blocking the action of aldosterone with MRAs.</p>\",\"PeriodicalId\":94329,\"journal\":{\"name\":\"Journal of clinical medicine research\",\"volume\":\"16 10\",\"pages\":\"509-517\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11557503/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of clinical medicine research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jocmr6058\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical medicine research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr6058","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
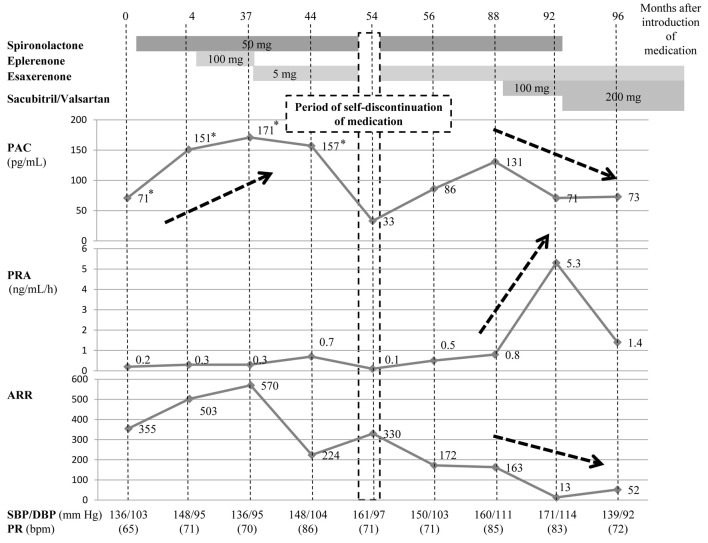
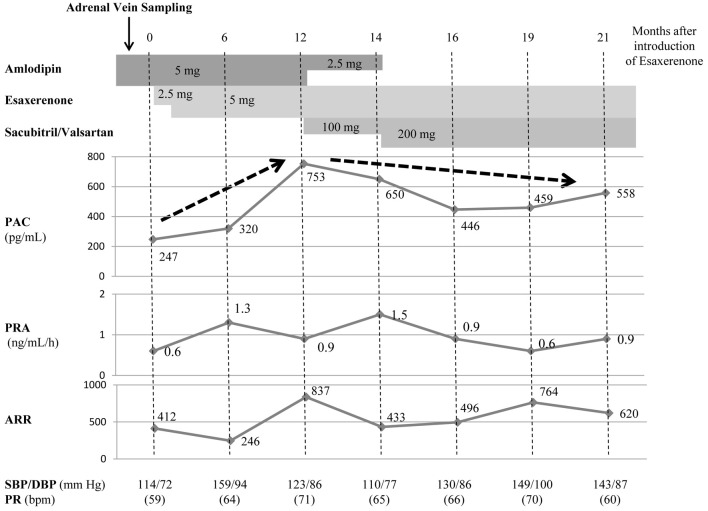
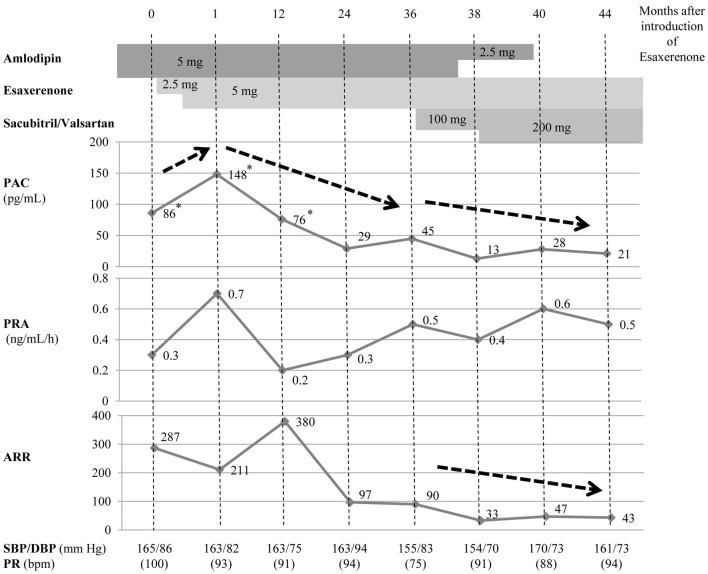
在原发性醛固酮增多症(PA)的药物治疗中,必须滴定矿质皮质激素受体拮抗剂(MRA)的剂量,以逆转高水平醛固酮引起的肾素抑制。然而,我们经常会遇到这样的病例:即使使用了最大剂量的 MRA,血浆肾素活性(PRA)也无法达到目标水平。在这种情况下,据报道,肾素酶抑制剂和血管紧张素 II 1 型受体阻滞剂的复方制剂 sacubitril/valsartan 可在体外和体内抑制醛固酮的分泌。如果萨库比特利/缬沙坦在这种情况下被证明有效,那么它可能会成为治疗 PA 的一种很有前景的方法。然而,关于在这种疾病中使用沙库比妥/缬沙坦的报道很少。我们对三名 PA 患者使用了附加的沙库比特利/缬沙坦,尽管他们服用了最大剂量的 MRA,但血压仍未得到充分降低,PRA 仍受到抑制。加用沙库比妥/缬沙坦后,血浆醛固酮浓度(PAC)的下降比 PRA 的上升更为明显。由于 MRA 并不抑制醛固酮的产生,而是通过阻断矿质皮质激素受体发挥作用,因此使用这些药物实际上会促进肾素-血管紧张素系统,并导致正反馈引起的 PAC 增高。服用 MRA 会导致 PAC 增加,而服用 sacubitril/valsartan 会导致 PAC 减少,这一现象的病理意义尚不清楚。对于 PA,使用沙库比妥/缬沙坦抑制醛固酮,并使用 MRA 阻断醛固酮的作用,可能会获得更有效的治疗。
Addition of Sacubitril/Valsartan to Mineralocorticoid Receptor Antagonist Therapy in Primary Aldosteronism: Effects on Plasma Aldosterone Concentration and Plasma Renin Activity.
In the pharmacologic treatment of primary aldosteronism (PA), titration of mineralocorticoid receptor antagonist (MRA) dosing is necessary to reverse the renin suppression caused by high aldosterone levels. However, we often encounter cases in which the plasma renin activity (PRA) does not achieve the target level, even with the maximum dose of MRA. In this setting, sacubitril/valsartan, a combination of a neprilysin inhibitor and an angiotensin II type 1 receptor blocker that is approved for use as adjunctive therapy with an MRA, has been reported to inhibit aldosterone secretion both in vitro and in vivo. If sacubitril/valsartan proves to be effective in this context, it may offer a promising treatment for PA. However, there are few reports on the use of sacubitril/valsartan in this disease. We used add-on sacubitril/valsartan in three patients with PA, in whom blood pressure was insufficiently reduced and PRA remained suppressed despite administering the maximum dose of MRA. With the addition of sacubitril/valsartan, the decrease in plasma aldosterone concentration (PAC) was more marked than the increase in PRA. Because MRAs do not suppress aldosterone production but instead act by blocking mineralocorticoid receptors, use of these agents actually promotes the renin-angiotensin system and leads to increased PAC resulting from positive feedback. The pathological significance of the phenomenon whereby PAC increases with MRA administration but decreases with the addition of sacubitril/valsartan is unclear. In PA, more effective treatment may be possible by suppressing aldosterone with sacubitril/valsartan and blocking the action of aldosterone with MRAs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


