Christopher L. Moore MD, Cary P. Gross MD, Louis Hart MD, Annette M. Molinaro PhD, Deborah Rhodes MD, Dinesh Singh MD, Cristiana Baloescu MD
{"title":"构建输尿管结石临床预测规则并提高其性能,无需考虑种族或民族因素:新的STONE评分。","authors":"Christopher L. Moore MD, Cary P. Gross MD, Louis Hart MD, Annette M. Molinaro PhD, Deborah Rhodes MD, Dinesh Singh MD, Cristiana Baloescu MD","doi":"10.1002/emp2.13324","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objectives</h3>\n \n <p>The original STONE score was designed to predict the presence of uncomplicated renal colic and the corresponding absence of alternate serious etiologies. It was retrospectively derived and prospectively validated and resulted in five variables: Sex (male gender), Timing (acute onset of pain), “Origin” (non-Black race), Nausea/vomiting (present), and Erythrocytes (microscopic hematuria). With recent increased awareness of the potential adverse impacts of including race (a socially constructed identity) in clinical prediction rules, we sought to determine if a revised STONE score without race could be constructed with similar diagnostic accuracy.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We used data from the original STONE score that utilized retrospective data on patients with confirmed kidney stone by computed tomography (CT) to derive a clinical prediction rule as well as prospective data to validate the score. These data were used to construct a revised STONE score after removing race as a variable. We performed univariate and multivariable logistic regression and compared the old and new STONE scores (including multivariable, integral, and three-level risk) using the area under the receiver operating characteristic curve (AUC) and misclassification rates.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>After the elimination of race, multivariable logistic regression revealed that gross hematuria was the next strongest feasible variable for the prediction of ureteral stone. This was incorporated into a revised STONE score by substituting “obvious hematuria” for “origin” (formerly race). The revised STONE score had similar predictive accuracy to the original STONE score: AUC 0.85 versus 0.86 (95% confidence interval [CI]: 0.82–0.87 and 0.79–0.93); misclassification rates were also unchanged, 0.23 versus 0.23 (95% CI: 0.20–0.25 and 0.20–0.25).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>We modified the STONE score to remove race and include “obvious hematuria” without losing clinical accuracy. Considering the potential adverse effects of propagating racial bias in clinical algorithms, we recommend using the revised STONE score. Future research could investigate the potential contributions of social drivers of health (SDOH) to the diagnosis of kidney stone.</p>\n </section>\n </div>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 6","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11543628/pdf/","citationCount":"0","resultStr":"{\"title\":\"Construction and performance of a clinical prediction rule for ureteral stone without the use of race or ethnicity: A new STONE score\",\"authors\":\"Christopher L. Moore MD, Cary P. Gross MD, Louis Hart MD, Annette M. Molinaro PhD, Deborah Rhodes MD, Dinesh Singh MD, Cristiana Baloescu MD\",\"doi\":\"10.1002/emp2.13324\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>The original STONE score was designed to predict the presence of uncomplicated renal colic and the corresponding absence of alternate serious etiologies. It was retrospectively derived and prospectively validated and resulted in five variables: Sex (male gender), Timing (acute onset of pain), “Origin” (non-Black race), Nausea/vomiting (present), and Erythrocytes (microscopic hematuria). With recent increased awareness of the potential adverse impacts of including race (a socially constructed identity) in clinical prediction rules, we sought to determine if a revised STONE score without race could be constructed with similar diagnostic accuracy.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We used data from the original STONE score that utilized retrospective data on patients with confirmed kidney stone by computed tomography (CT) to derive a clinical prediction rule as well as prospective data to validate the score. These data were used to construct a revised STONE score after removing race as a variable. We performed univariate and multivariable logistic regression and compared the old and new STONE scores (including multivariable, integral, and three-level risk) using the area under the receiver operating characteristic curve (AUC) and misclassification rates.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>After the elimination of race, multivariable logistic regression revealed that gross hematuria was the next strongest feasible variable for the prediction of ureteral stone. This was incorporated into a revised STONE score by substituting “obvious hematuria” for “origin” (formerly race). The revised STONE score had similar predictive accuracy to the original STONE score: AUC 0.85 versus 0.86 (95% confidence interval [CI]: 0.82–0.87 and 0.79–0.93); misclassification rates were also unchanged, 0.23 versus 0.23 (95% CI: 0.20–0.25 and 0.20–0.25).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>We modified the STONE score to remove race and include “obvious hematuria” without losing clinical accuracy. Considering the potential adverse effects of propagating racial bias in clinical algorithms, we recommend using the revised STONE score. Future research could investigate the potential contributions of social drivers of health (SDOH) to the diagnosis of kidney stone.</p>\\n </section>\\n </div>\",\"PeriodicalId\":73967,\"journal\":{\"name\":\"Journal of the American College of Emergency Physicians open\",\"volume\":\"5 6\",\"pages\":\"\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-11-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11543628/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American College of Emergency Physicians open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13324\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13324","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
目的:最初的 STONE 评分旨在预测是否存在无并发症的肾绞痛以及是否存在其他严重病因。它通过回顾性分析和前瞻性验证得出了五个变量:性别(男性)、时间(急性疼痛发作)、"出身"(非黑人种族)、恶心/呕吐(出现)和红细胞(镜下血尿)。最近,人们越来越意识到在临床预测规则中加入种族(一种社会建构的身份)可能会产生不利影响,因此我们试图确定是否可以构建一个不含种族的修订版 STONE 评分,并具有类似的诊断准确性:我们使用了原始 STONE 评分的数据,该评分利用计算机断层扫描(CT)确诊肾结石患者的回顾性数据来推导临床预测规则,并利用前瞻性数据来验证该评分。在剔除种族这一变量后,我们利用这些数据构建了经修订的 STONE 评分。我们进行了单变量和多变量逻辑回归,并使用接收者操作特征曲线下面积(AUC)和误诊率比较了新旧 STONE 评分(包括多变量、积分和三级风险):排除种族因素后,多变量逻辑回归显示,毛血尿是预测输尿管结石的第二大可行变量。通过用 "明显血尿 "代替 "出身"(以前的种族),将这一变量纳入了修订后的 STONE 评分。修订后的 STONE 评分与最初的 STONE 评分具有相似的预测准确性:AUC为0.85对0.86(95%置信区间[CI]:0.82-0.87和0.79-0.93);误诊率也没有变化,为0.23对0.23(95%置信区间:0.20-0.25和0.20-0.25):我们对 STONE 评分进行了修改,删除了种族因素并纳入了 "明显血尿",但并没有降低临床准确性。考虑到在临床算法中传播种族偏见的潜在不利影响,我们建议使用修订后的 STONE 评分。未来的研究可以调查社会健康驱动因素(SDOH)对肾结石诊断的潜在影响。
Construction and performance of a clinical prediction rule for ureteral stone without the use of race or ethnicity: A new STONE score
Objectives
The original STONE score was designed to predict the presence of uncomplicated renal colic and the corresponding absence of alternate serious etiologies. It was retrospectively derived and prospectively validated and resulted in five variables: Sex (male gender), Timing (acute onset of pain), “Origin” (non-Black race), Nausea/vomiting (present), and Erythrocytes (microscopic hematuria). With recent increased awareness of the potential adverse impacts of including race (a socially constructed identity) in clinical prediction rules, we sought to determine if a revised STONE score without race could be constructed with similar diagnostic accuracy.
Methods
We used data from the original STONE score that utilized retrospective data on patients with confirmed kidney stone by computed tomography (CT) to derive a clinical prediction rule as well as prospective data to validate the score. These data were used to construct a revised STONE score after removing race as a variable. We performed univariate and multivariable logistic regression and compared the old and new STONE scores (including multivariable, integral, and three-level risk) using the area under the receiver operating characteristic curve (AUC) and misclassification rates.
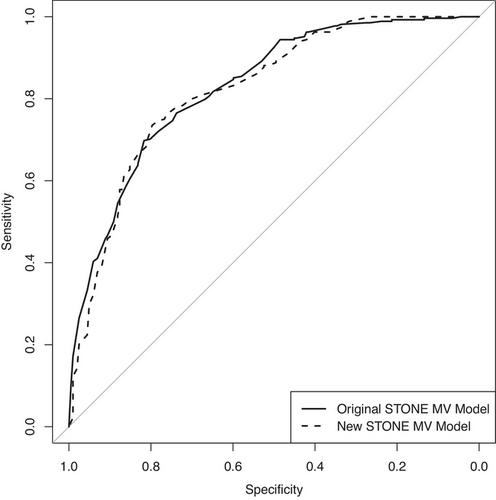
Results
After the elimination of race, multivariable logistic regression revealed that gross hematuria was the next strongest feasible variable for the prediction of ureteral stone. This was incorporated into a revised STONE score by substituting “obvious hematuria” for “origin” (formerly race). The revised STONE score had similar predictive accuracy to the original STONE score: AUC 0.85 versus 0.86 (95% confidence interval [CI]: 0.82–0.87 and 0.79–0.93); misclassification rates were also unchanged, 0.23 versus 0.23 (95% CI: 0.20–0.25 and 0.20–0.25).
Conclusions
We modified the STONE score to remove race and include “obvious hematuria” without losing clinical accuracy. Considering the potential adverse effects of propagating racial bias in clinical algorithms, we recommend using the revised STONE score. Future research could investigate the potential contributions of social drivers of health (SDOH) to the diagnosis of kidney stone.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


