Ali H. Zahalka, Ethan Fram, Evan Garden, Lauren Howard, Emily Wiggins, Mustufa Babar, Jay Annam, Allison Reagan, Benjamin Eilender, Amanda de Hoedt, Stephen J. Freedland, Ash Tewari, Kara L. Watts
{"title":"使用β-受体阻滞剂阿替洛尔与前列腺癌主动监测升级之间的关系。","authors":"Ali H. Zahalka, Ethan Fram, Evan Garden, Lauren Howard, Emily Wiggins, Mustufa Babar, Jay Annam, Allison Reagan, Benjamin Eilender, Amanda de Hoedt, Stephen J. Freedland, Ash Tewari, Kara L. Watts","doi":"10.1002/bco2.441","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objectives</h3>\n \n <p>The objective of this study is to investigate the association between the use of beta-adrenergic antagonist atenolol and risk of pathologic upgrade in patients on active surveillance, considering growing literature implicating adrenergic innervation with disease progression mediated through beta-adrenergic signalling.</p>\n </section>\n \n <section>\n \n <h3> Patients and Methods</h3>\n \n <p>Men with low-risk or favourable intermediate-risk prostate cancer who were placed on an active surveillance protocol between 2006 and 2020 across three diverse urban hospitals were included. Exposure was duration of atenolol use, and outcome was pathologic grade group upgrading (to GG ≥ 3) on final prostate biopsy. Cox proportional hazard regression models were used to determine the associations between atenolol use and risk of upgrading with time, on a per-examination basis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 467 men with initial GG ≤ 2 were included. Postdiagnosis atenolol use was associated with a decreased risk of pathologic upgrade to GG ≥ 3 on final repeat biopsy (HR 0.81, 95% CI 0.39–0.98). Longer duration of postdiagnosis atenolol use (>2 years) and greater cumulative atenolol dose (>730 defined daily doses) were associated with a more pronounced decreased risk of upgrade to GG ≥ 3 (HR 0.41, 95% CI 0.05–0.88, and HR 0.32, 95% CI 0.15–0.99, respectively). Initiation of atenolol use prior to prostate cancer diagnosis had a slightly greater protective effect than drug initiation postdiagnosis (HR 0.79, 95% CI 0.43–0.98, and HR 0.83, 95% CI 0.30–0.99, respectively).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Beta-adrenergic blockade with atenolol use in men on active surveillance is associated with a reduced risk for clinically significant grade group pathologic upgrade.</p>\n </section>\n </div>","PeriodicalId":72420,"journal":{"name":"BJUI compass","volume":"5 11","pages":"1095-1100"},"PeriodicalIF":1.6000,"publicationDate":"2024-10-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11557265/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association between beta-blocker atenolol use and prostate cancer upgrading in active surveillance†\",\"authors\":\"Ali H. Zahalka, Ethan Fram, Evan Garden, Lauren Howard, Emily Wiggins, Mustufa Babar, Jay Annam, Allison Reagan, Benjamin Eilender, Amanda de Hoedt, Stephen J. Freedland, Ash Tewari, Kara L. Watts\",\"doi\":\"10.1002/bco2.441\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>The objective of this study is to investigate the association between the use of beta-adrenergic antagonist atenolol and risk of pathologic upgrade in patients on active surveillance, considering growing literature implicating adrenergic innervation with disease progression mediated through beta-adrenergic signalling.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Patients and Methods</h3>\\n \\n <p>Men with low-risk or favourable intermediate-risk prostate cancer who were placed on an active surveillance protocol between 2006 and 2020 across three diverse urban hospitals were included. Exposure was duration of atenolol use, and outcome was pathologic grade group upgrading (to GG ≥ 3) on final prostate biopsy. Cox proportional hazard regression models were used to determine the associations between atenolol use and risk of upgrading with time, on a per-examination basis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 467 men with initial GG ≤ 2 were included. Postdiagnosis atenolol use was associated with a decreased risk of pathologic upgrade to GG ≥ 3 on final repeat biopsy (HR 0.81, 95% CI 0.39–0.98). Longer duration of postdiagnosis atenolol use (>2 years) and greater cumulative atenolol dose (>730 defined daily doses) were associated with a more pronounced decreased risk of upgrade to GG ≥ 3 (HR 0.41, 95% CI 0.05–0.88, and HR 0.32, 95% CI 0.15–0.99, respectively). Initiation of atenolol use prior to prostate cancer diagnosis had a slightly greater protective effect than drug initiation postdiagnosis (HR 0.79, 95% CI 0.43–0.98, and HR 0.83, 95% CI 0.30–0.99, respectively).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Beta-adrenergic blockade with atenolol use in men on active surveillance is associated with a reduced risk for clinically significant grade group pathologic upgrade.</p>\\n </section>\\n </div>\",\"PeriodicalId\":72420,\"journal\":{\"name\":\"BJUI compass\",\"volume\":\"5 11\",\"pages\":\"1095-1100\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2024-10-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11557265/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BJUI compass\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/bco2.441\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJUI compass","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/bco2.441","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
研究目的考虑到越来越多的文献表明肾上腺素能神经支配通过β-肾上腺素能信号介导疾病进展,本研究旨在调查主动监测患者使用β-肾上腺素能拮抗剂阿替洛尔与病理升级风险之间的关系:纳入了三家不同城市医院在 2006 年至 2020 年期间接受主动监测方案的低危或良好中危前列腺癌男性患者。暴露是指阿替洛尔的使用时间,结果是指最终前列腺活检的病理分级组别升级(GG≥3)。采用Cox比例危险回归模型确定阿替洛尔的使用与每次检查的升级风险之间的关系:结果:共纳入467名初始GG≤2的男性。诊断后使用阿替洛尔与最终重复活检时病理结果升级为GG≥3的风险降低有关(HR 0.81,95% CI 0.39-0.98)。诊断后使用阿替洛尔的时间越长(>2 年),阿替洛尔的累积剂量越大(>730 定义日剂量),升级为 GG ≥ 3 的风险就越低(HR 分别为 0.41,95% CI 0.05-0.88 和 HR 0.32,95% CI 0.15-0.99)。前列腺癌确诊前开始使用阿替洛尔的保护作用略大于确诊后开始用药(分别为HR 0.79,95% CI 0.43-0.98和HR 0.83,95% CI 0.30-0.99):结论:在接受主动监测的男性中使用阿替洛尔进行β-肾上腺素能阻断与降低临床上显著的病理分级升级风险有关。
Association between beta-blocker atenolol use and prostate cancer upgrading in active surveillance†
Objectives
The objective of this study is to investigate the association between the use of beta-adrenergic antagonist atenolol and risk of pathologic upgrade in patients on active surveillance, considering growing literature implicating adrenergic innervation with disease progression mediated through beta-adrenergic signalling.
Patients and Methods
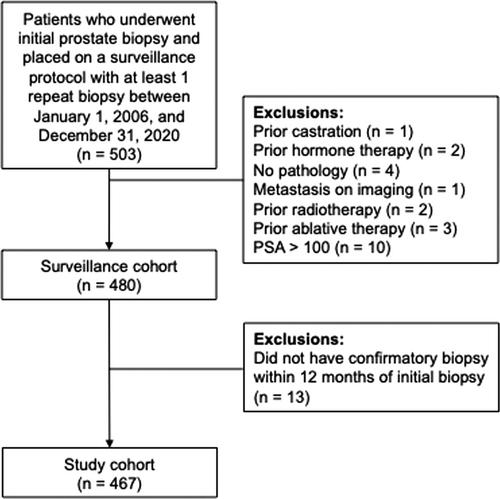
Men with low-risk or favourable intermediate-risk prostate cancer who were placed on an active surveillance protocol between 2006 and 2020 across three diverse urban hospitals were included. Exposure was duration of atenolol use, and outcome was pathologic grade group upgrading (to GG ≥ 3) on final prostate biopsy. Cox proportional hazard regression models were used to determine the associations between atenolol use and risk of upgrading with time, on a per-examination basis.
Results
A total of 467 men with initial GG ≤ 2 were included. Postdiagnosis atenolol use was associated with a decreased risk of pathologic upgrade to GG ≥ 3 on final repeat biopsy (HR 0.81, 95% CI 0.39–0.98). Longer duration of postdiagnosis atenolol use (>2 years) and greater cumulative atenolol dose (>730 defined daily doses) were associated with a more pronounced decreased risk of upgrade to GG ≥ 3 (HR 0.41, 95% CI 0.05–0.88, and HR 0.32, 95% CI 0.15–0.99, respectively). Initiation of atenolol use prior to prostate cancer diagnosis had a slightly greater protective effect than drug initiation postdiagnosis (HR 0.79, 95% CI 0.43–0.98, and HR 0.83, 95% CI 0.30–0.99, respectively).
Conclusions
Beta-adrenergic blockade with atenolol use in men on active surveillance is associated with a reduced risk for clinically significant grade group pathologic upgrade.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


