Marc Brisson, Jean-François Laprise, Mélanie Drolet, Éléonore Chamberland, Élodie Bénard, Emily A Burger, Mark Jit, Jane J Kim, Lauri E Markowitz, Chantal Sauvageau, Stephen Sy
{"title":"高收入国家改用 1 剂人类乳头瘤病毒疫苗接种对人口的影响:利用数学建模研究不确定性。","authors":"Marc Brisson, Jean-François Laprise, Mélanie Drolet, Éléonore Chamberland, Élodie Bénard, Emily A Burger, Mark Jit, Jane J Kim, Lauri E Markowitz, Chantal Sauvageau, Stephen Sy","doi":"10.1093/jncimonographs/lgae038","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A concern in high-income countries is that switching to 1-dose human papillomavirus (HPV) vaccination could cause a rebound in HPV infection and cervical cancer if 1-dose efficacy or duration were inferior to 2 doses. Using mathematical modeling and up-to-date trial-based data, we projected the population-level effectiveness of switching from 2-dose to 1-dose vaccination under different vaccine efficacy and duration assumptions in high-income countries.</p><p><strong>Methods: </strong>We used HPV-ADVISE (Agent-based Dynamic model for VaccInation and Screening Evaluation), a transmission-dynamic model of HPV infection and cervical cancer, varying key model assumptions to identify those with the greatest impact on projections of HPV-16 and cervical cancer incidence over time: 1) 1-dose vaccine efficacy and vaccine duration, 2) mechanisms of vaccine efficacy and duration over time, 3) midadult (>30 years of age) sexual behavior, 4) progression to cervical cancer among midadults, and 5) vaccination coverage and programs.</p><p><strong>Results: </strong>In high-income countries, 1-dose vaccination would cause no appreciable rebound in HPV-16 infection, except for a limited rebound under the most pessimistic assumptions of vaccine duration (average, 25 years), because 1) the switch would occur when HPV prevalence is low because of high 2-dose vaccination coverage and 2) individuals would be protected during their peak ages of sexual activity (<35 to 40 years of age). Our model projects a more limited rebound in cervical cancer because of a shift to older age at infection, resulting in fewer life-years left to potentially develop cancer. Projections were robust when varying key model assumptions.</p><p><strong>Conclusions: </strong>High protection during peak ages of sexual activity in high-income countries would likely mitigate any potential rebounds in HPV infection and cervical cancer under the most pessimistic assumptions of 1-dose efficacy and duration.</p>","PeriodicalId":73988,"journal":{"name":"Journal of the National Cancer Institute. Monographs","volume":"2024 67","pages":"387-399"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11555275/pdf/","citationCount":"0","resultStr":"{\"title\":\"Population-level impact of switching to 1-dose human papillomavirus vaccination in high-income countries: examining uncertainties using mathematical modeling.\",\"authors\":\"Marc Brisson, Jean-François Laprise, Mélanie Drolet, Éléonore Chamberland, Élodie Bénard, Emily A Burger, Mark Jit, Jane J Kim, Lauri E Markowitz, Chantal Sauvageau, Stephen Sy\",\"doi\":\"10.1093/jncimonographs/lgae038\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A concern in high-income countries is that switching to 1-dose human papillomavirus (HPV) vaccination could cause a rebound in HPV infection and cervical cancer if 1-dose efficacy or duration were inferior to 2 doses. Using mathematical modeling and up-to-date trial-based data, we projected the population-level effectiveness of switching from 2-dose to 1-dose vaccination under different vaccine efficacy and duration assumptions in high-income countries.</p><p><strong>Methods: </strong>We used HPV-ADVISE (Agent-based Dynamic model for VaccInation and Screening Evaluation), a transmission-dynamic model of HPV infection and cervical cancer, varying key model assumptions to identify those with the greatest impact on projections of HPV-16 and cervical cancer incidence over time: 1) 1-dose vaccine efficacy and vaccine duration, 2) mechanisms of vaccine efficacy and duration over time, 3) midadult (>30 years of age) sexual behavior, 4) progression to cervical cancer among midadults, and 5) vaccination coverage and programs.</p><p><strong>Results: </strong>In high-income countries, 1-dose vaccination would cause no appreciable rebound in HPV-16 infection, except for a limited rebound under the most pessimistic assumptions of vaccine duration (average, 25 years), because 1) the switch would occur when HPV prevalence is low because of high 2-dose vaccination coverage and 2) individuals would be protected during their peak ages of sexual activity (<35 to 40 years of age). Our model projects a more limited rebound in cervical cancer because of a shift to older age at infection, resulting in fewer life-years left to potentially develop cancer. Projections were robust when varying key model assumptions.</p><p><strong>Conclusions: </strong>High protection during peak ages of sexual activity in high-income countries would likely mitigate any potential rebounds in HPV infection and cervical cancer under the most pessimistic assumptions of 1-dose efficacy and duration.</p>\",\"PeriodicalId\":73988,\"journal\":{\"name\":\"Journal of the National Cancer Institute. Monographs\",\"volume\":\"2024 67\",\"pages\":\"387-399\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11555275/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the National Cancer Institute. Monographs\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/jncimonographs/lgae038\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the National Cancer Institute. Monographs","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jncimonographs/lgae038","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Population-level impact of switching to 1-dose human papillomavirus vaccination in high-income countries: examining uncertainties using mathematical modeling.
Background: A concern in high-income countries is that switching to 1-dose human papillomavirus (HPV) vaccination could cause a rebound in HPV infection and cervical cancer if 1-dose efficacy or duration were inferior to 2 doses. Using mathematical modeling and up-to-date trial-based data, we projected the population-level effectiveness of switching from 2-dose to 1-dose vaccination under different vaccine efficacy and duration assumptions in high-income countries.
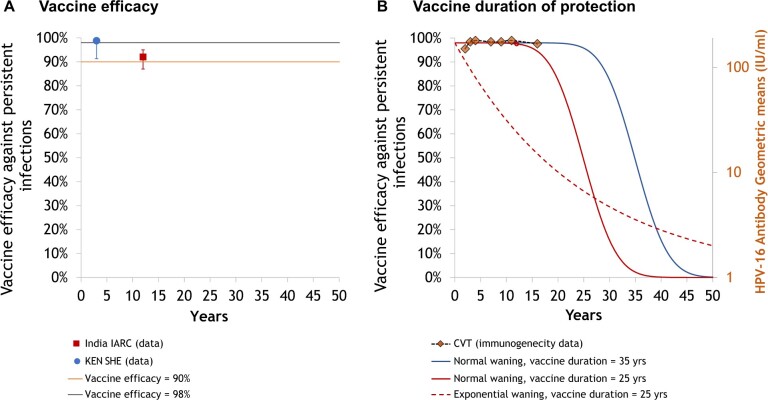
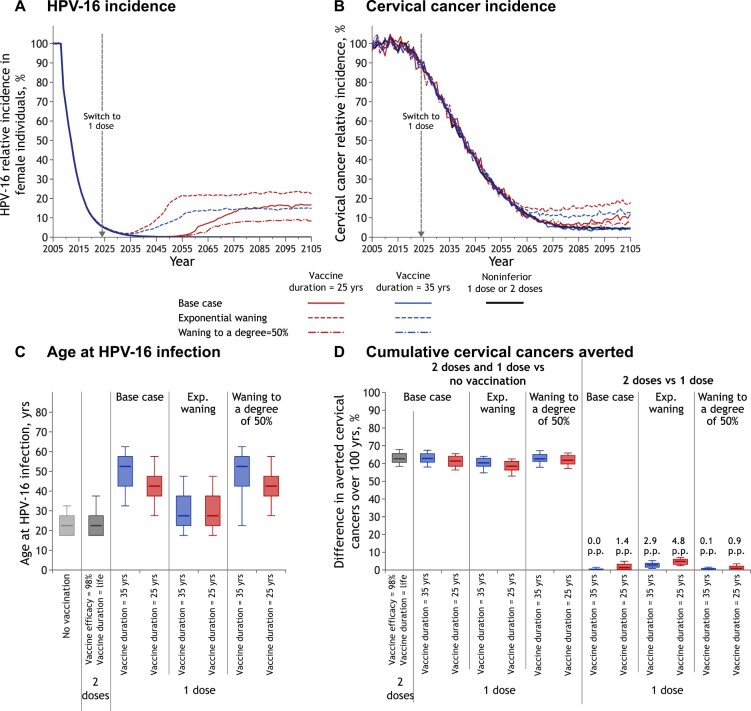
Methods: We used HPV-ADVISE (Agent-based Dynamic model for VaccInation and Screening Evaluation), a transmission-dynamic model of HPV infection and cervical cancer, varying key model assumptions to identify those with the greatest impact on projections of HPV-16 and cervical cancer incidence over time: 1) 1-dose vaccine efficacy and vaccine duration, 2) mechanisms of vaccine efficacy and duration over time, 3) midadult (>30 years of age) sexual behavior, 4) progression to cervical cancer among midadults, and 5) vaccination coverage and programs.
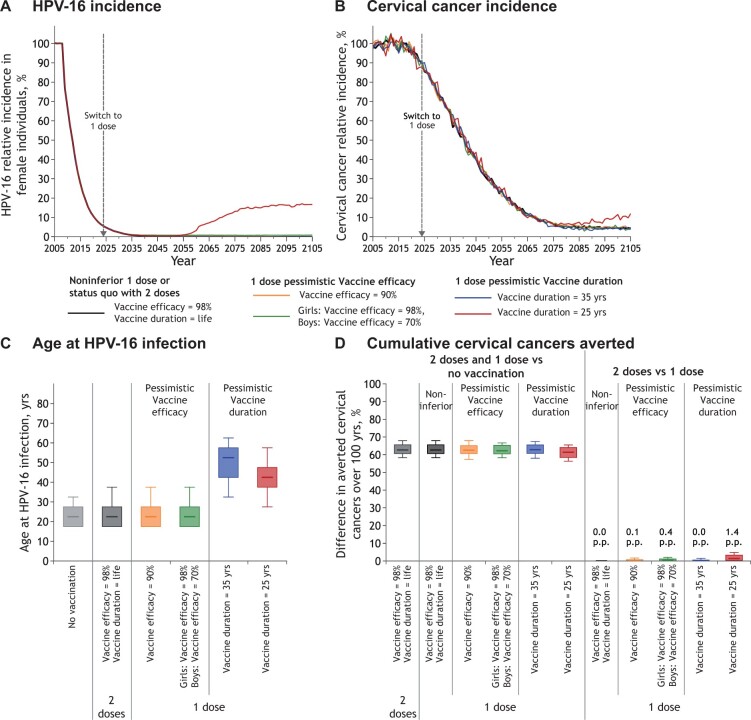
Results: In high-income countries, 1-dose vaccination would cause no appreciable rebound in HPV-16 infection, except for a limited rebound under the most pessimistic assumptions of vaccine duration (average, 25 years), because 1) the switch would occur when HPV prevalence is low because of high 2-dose vaccination coverage and 2) individuals would be protected during their peak ages of sexual activity (<35 to 40 years of age). Our model projects a more limited rebound in cervical cancer because of a shift to older age at infection, resulting in fewer life-years left to potentially develop cancer. Projections were robust when varying key model assumptions.
Conclusions: High protection during peak ages of sexual activity in high-income countries would likely mitigate any potential rebounds in HPV infection and cervical cancer under the most pessimistic assumptions of 1-dose efficacy and duration.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


