{"title":"无诊断性经皮肝肿瘤活检的风险因素:根据错误原因对938例活检进行的单中心回顾性分析。","authors":"Shintaro Kimura, Miyuki Sone, Shunsuke Sugawara, Chihiro Itou, Takumi Oshima, Mizuki Ozawa, Rakuhei Nakama, Sho Murakami, Yoshiyuki Matsui, Yasuaki Arai, Masahiko Kusumoto","doi":"10.1007/s11604-024-01703-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To evaluate the risk factors of non-diagnostic results based on cause of error in liver tumor biopsy.</p><p><strong>Materials and methods: </strong>This single-institution, retrospective study included 843 patients [445 men, 398 women; median age, 67 years] who underwent a total of 938 liver tumor biopsies between April 2018 and September 2022. An 18-G cutting biopsy needle with a 17-G introducer needle was used. Ultrasound was used as the first choice for image guidance, and computed tomography was alternatively or complementarily used only for tumors with poor ultrasound visibility. Non-diagnostic biopsies were divided into two groups depending on the cause of error, either technical or targeting error. Biopsies in which the biopsy needle did not hit the target tumor were classified as technical error. Biopsies in which insufficient tissue was obtained due to necrosis or degeneration despite the biopsy needle hitting the target tumor were classified as targeting error. This classification was based on pre-procedural enhanced-imaging, intro-procedural imaging, and pathological findings. Statistical analysis was performed using binary logistic regression.</p><p><strong>Results: </strong>The non-diagnostic rate was 4.6%. Twenty-six and seventeen biopsies were classified as technical and targeting errors, respectively. In the technical error group, tumor size ≤ 17 mm and computed tomography-assisted biopsy due to poor ultrasound visibility were identified as risk factors (p < 0.001 and p = 0.021, respectively), and the tumors with both factors had a significantly high risk of technical error compared to those without both factors (non-diagnostic rate: 17.2 vs 1.1%, p < 0.001). In the targeting error group, tumor size ≥ 42 mm was identified as a risk factor (p = 0.003).</p><p><strong>Conclusion: </strong>Tumor size ≤ 17 mm and computed tomography-assisted biopsy due to poor ultrasound visibility were risk factors for technical error, and tumor size ≥ 42 mm was a risk factor for targeting error in liver tumor biopsies.</p>","PeriodicalId":14691,"journal":{"name":"Japanese Journal of Radiology","volume":" ","pages":"696-705"},"PeriodicalIF":2.1000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11953201/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk factors of non-diagnostic percutaneous liver tumor biopsy: a single-center retrospective analysis of 938 biopsies based on cause of error.\",\"authors\":\"Shintaro Kimura, Miyuki Sone, Shunsuke Sugawara, Chihiro Itou, Takumi Oshima, Mizuki Ozawa, Rakuhei Nakama, Sho Murakami, Yoshiyuki Matsui, Yasuaki Arai, Masahiko Kusumoto\",\"doi\":\"10.1007/s11604-024-01703-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To evaluate the risk factors of non-diagnostic results based on cause of error in liver tumor biopsy.</p><p><strong>Materials and methods: </strong>This single-institution, retrospective study included 843 patients [445 men, 398 women; median age, 67 years] who underwent a total of 938 liver tumor biopsies between April 2018 and September 2022. An 18-G cutting biopsy needle with a 17-G introducer needle was used. Ultrasound was used as the first choice for image guidance, and computed tomography was alternatively or complementarily used only for tumors with poor ultrasound visibility. Non-diagnostic biopsies were divided into two groups depending on the cause of error, either technical or targeting error. Biopsies in which the biopsy needle did not hit the target tumor were classified as technical error. Biopsies in which insufficient tissue was obtained due to necrosis or degeneration despite the biopsy needle hitting the target tumor were classified as targeting error. This classification was based on pre-procedural enhanced-imaging, intro-procedural imaging, and pathological findings. Statistical analysis was performed using binary logistic regression.</p><p><strong>Results: </strong>The non-diagnostic rate was 4.6%. Twenty-six and seventeen biopsies were classified as technical and targeting errors, respectively. In the technical error group, tumor size ≤ 17 mm and computed tomography-assisted biopsy due to poor ultrasound visibility were identified as risk factors (p < 0.001 and p = 0.021, respectively), and the tumors with both factors had a significantly high risk of technical error compared to those without both factors (non-diagnostic rate: 17.2 vs 1.1%, p < 0.001). In the targeting error group, tumor size ≥ 42 mm was identified as a risk factor (p = 0.003).</p><p><strong>Conclusion: </strong>Tumor size ≤ 17 mm and computed tomography-assisted biopsy due to poor ultrasound visibility were risk factors for technical error, and tumor size ≥ 42 mm was a risk factor for targeting error in liver tumor biopsies.</p>\",\"PeriodicalId\":14691,\"journal\":{\"name\":\"Japanese Journal of Radiology\",\"volume\":\" \",\"pages\":\"696-705\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11953201/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Japanese Journal of Radiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11604-024-01703-3\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Japanese Journal of Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11604-024-01703-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/14 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Risk factors of non-diagnostic percutaneous liver tumor biopsy: a single-center retrospective analysis of 938 biopsies based on cause of error.
Purpose: To evaluate the risk factors of non-diagnostic results based on cause of error in liver tumor biopsy.
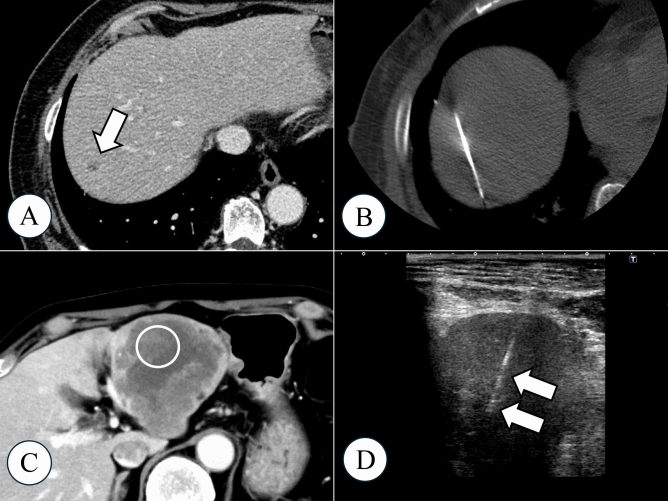
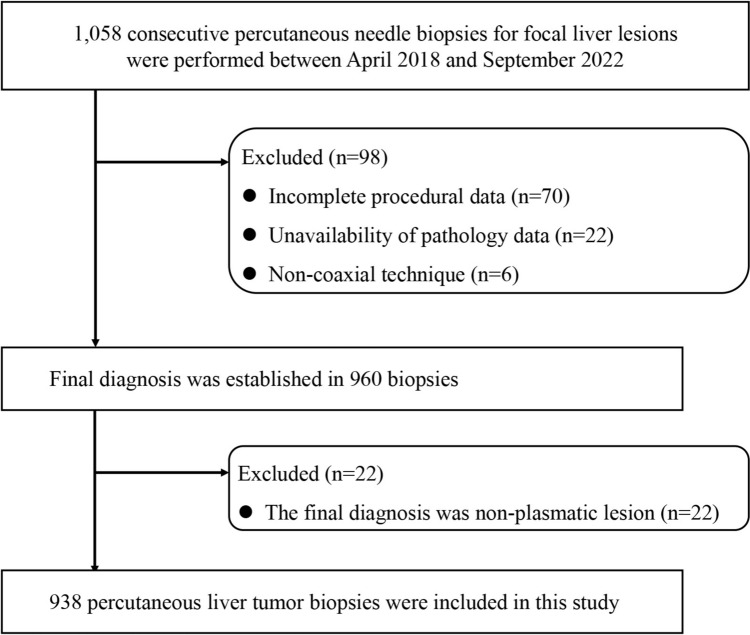
Materials and methods: This single-institution, retrospective study included 843 patients [445 men, 398 women; median age, 67 years] who underwent a total of 938 liver tumor biopsies between April 2018 and September 2022. An 18-G cutting biopsy needle with a 17-G introducer needle was used. Ultrasound was used as the first choice for image guidance, and computed tomography was alternatively or complementarily used only for tumors with poor ultrasound visibility. Non-diagnostic biopsies were divided into two groups depending on the cause of error, either technical or targeting error. Biopsies in which the biopsy needle did not hit the target tumor were classified as technical error. Biopsies in which insufficient tissue was obtained due to necrosis or degeneration despite the biopsy needle hitting the target tumor were classified as targeting error. This classification was based on pre-procedural enhanced-imaging, intro-procedural imaging, and pathological findings. Statistical analysis was performed using binary logistic regression.
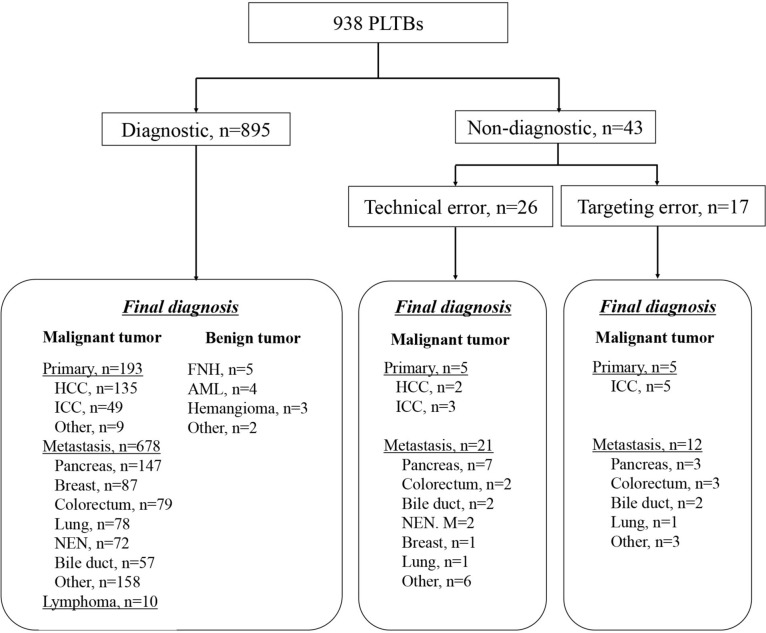
Results: The non-diagnostic rate was 4.6%. Twenty-six and seventeen biopsies were classified as technical and targeting errors, respectively. In the technical error group, tumor size ≤ 17 mm and computed tomography-assisted biopsy due to poor ultrasound visibility were identified as risk factors (p < 0.001 and p = 0.021, respectively), and the tumors with both factors had a significantly high risk of technical error compared to those without both factors (non-diagnostic rate: 17.2 vs 1.1%, p < 0.001). In the targeting error group, tumor size ≥ 42 mm was identified as a risk factor (p = 0.003).
Conclusion: Tumor size ≤ 17 mm and computed tomography-assisted biopsy due to poor ultrasound visibility were risk factors for technical error, and tumor size ≥ 42 mm was a risk factor for targeting error in liver tumor biopsies.
期刊介绍:
Japanese Journal of Radiology is a peer-reviewed journal, officially published by the Japan Radiological Society. The main purpose of the journal is to provide a forum for the publication of papers documenting recent advances and new developments in the field of radiology in medicine and biology. The scope of Japanese Journal of Radiology encompasses but is not restricted to diagnostic radiology, interventional radiology, radiation oncology, nuclear medicine, radiation physics, and radiation biology. Additionally, the journal covers technical and industrial innovations. The journal welcomes original articles, technical notes, review articles, pictorial essays and letters to the editor. The journal also provides announcements from the boards and the committees of the society. Membership in the Japan Radiological Society is not a prerequisite for submission. Contributions are welcomed from all parts of the world.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



