Sabrina Setembre Batah, Andrea Jazel Rodriguez-Herrera, Maria Júlia Faci do Marco, Juliana Rocha Souza Chiappetto, Mariana Gatto, Simone Alves do Vale, Robson Aparecido Prudente, Amanda Piveta Schnepper, Robson Francisco Carvalho, João Paulo Facio Almeida, Tales Rubens de Nadai, Marcel Konigkam Santos, Li Siyuan Wada, José Baddini-Martinez, Danilo Tadao Wada, Andrea Antunes Cetlin, Vera Luiza Capelozzi, Bruno Guedes Baldi, Suzana Tanni, Rosane Duarte Achcar, Alexandre Todorovic Fabro
{"title":"转录组分析揭示了2019年冠状病毒病后肺纤维化与纤维化进展相关的基因表达动态。","authors":"Sabrina Setembre Batah, Andrea Jazel Rodriguez-Herrera, Maria Júlia Faci do Marco, Juliana Rocha Souza Chiappetto, Mariana Gatto, Simone Alves do Vale, Robson Aparecido Prudente, Amanda Piveta Schnepper, Robson Francisco Carvalho, João Paulo Facio Almeida, Tales Rubens de Nadai, Marcel Konigkam Santos, Li Siyuan Wada, José Baddini-Martinez, Danilo Tadao Wada, Andrea Antunes Cetlin, Vera Luiza Capelozzi, Bruno Guedes Baldi, Suzana Tanni, Rosane Duarte Achcar, Alexandre Todorovic Fabro","doi":"10.1002/ctm2.70088","DOIUrl":null,"url":null,"abstract":"<p>Dear Editor,</p><p>Our study has identified a gene expression profile associated with the progression of coronavirus disease 2019 (COVID-19) to pulmonary fibrosis in a pro-fibrotic environment similar to that found in fibrosing interstitial lung diseases (f-ILDs). Briefly, we noted the common expression of 86 genes in post-COVID-19 pulmonary fibrosis (post-CPF) and f-ILDs, indicating their likely involvement in perpetuating pulmonary fibrosis through shared fibrotic pathways—confirmed by the in-situ expression of MUC5ac and WNT10a. Furthermore, an additional set of 31 genes exhibited common expression patterns between subacute COVID-19, the so-called organizing diffuse alveolar damage (ODAD), and CPF, as well as f-ILDs. Among those genes, MUC4 and KRT5 were confirmed by immunohistochemistry, suggesting their role as potential predictors for the early outcome of possible pulmonary fibrosis.</p><p>Post-CPF is a long-term complication diagnosed by clinical setting, pulmonary function tests and/or image examinations.<span><sup>1</sup></span> Initially, some COVID-19-infected patients develop acute respiratory distress syndrome (ARDS) during the exudative phase of DAD, marked by cytokine storm and immune cell recruitment.<span><sup>2</sup></span> Following the inflammatory peak and pneumocyte injury, myofibroblast activation triggers extracellular matrix (ECM) deposition, leading to ODAD-phase which typically restores to typical lung architecture. However, some patients progress to pulmonary fibrosis<span><sup>3</sup></span> with morphological changes that are driven by a complex pathophysiological sequence and dynamic gene expression shifts. In the end, the fibrotic outcome can resemble other f-ILDs. Identifying gene expression levels linked to the progression from ODAD to CPF is crucial for finding biomarkers for early diagnosis. Our study aimed to identify potential biomarkers in gene expression associated with fibrotic progression to CPF by analyzing the transcriptome of patients with ODAD, CPF, f-ILDs and controls.</p><p>As previously described by Batah et al.,<span><sup>4</sup></span> autopsies from the ODAD group revealed ODAD-phase with bronchiolar metaplasia, myxoid fibrosis, myofibroblastic activation and extensive alveolar septal thickening with collagen types I and III deposition (Table S1; Figure 1A–C). Meanwhile, after an average of 324.6 days following the initial positive nasopharyngeal swab for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), patients from the CPF group developed pulmonary fibrosis with bronchiolar metaplasia and parenchymal remodelling with increased collagen deposition, especially type I (suppinfo1; Figure 1D–F). Although the common remodelling profile, the differential gene expression (DGE) analysis between ODAD and CPF revealed distinct gene signatures (Figure S1A,B), Some of the top 20 DGEs reflect the manifestation of ARDS in ODAD patients (Figure S1C,D and Table S2). For example, the upregulation of SERPINE1 -fibrinolysis inhibitor- in ODAD suggests the accumulation of deposited fibrin as a better pathophysiological response to SARS-CoV-2.<span><sup>5</sup></span> However, as mentioned earlier, both groups revealed parenchymal remodelling, and the WP Lung Fibrosis gene set (GSEA systematic name M39477) highlighted only a few DGE between the groups: upregulated MMP9 and TERT and downregulated MUC5B and FGF1 in ODAD compared to CPF (Figure S1E and Table S3). Therefore, some fibrotic pathways might be present in both groups, suggesting a possible similarity with the transcriptomic profile of f-ILD patients.</p><p>In fact, our data revealed a significant similarity in gene expression among the groups compared to f-ILD, presenting dense fibrosis, architectural distortion, bronchiolar metaplasia, fibroblast foci and collagen types I and III deposition (Table S1 and Figure 1G–I). The similarity is seen by the overlap of cases in the paired DGE analyses between CPF versus f-ILD (Figure S2A,B) and ODAD versus f-ILD (Figure S3A,B). In both principal component analyses, f-ILD patients were divided into two distinct clusters: In Figure S2A, Cluster A is distinct from the other cases, while Cluster B is found among the CPF patients. Cluster A displays a bronchiolocentric remodelling pattern, whereas Cluster B exhibits a non-specific lesion pattern characterized by uniform thickening of the pulmonary interstitium, similar to that observed in CPF patients. Similarly, in Figure S3A, Cluster D has the same patients as Cluster A, who also exhibit bronchiolocentric ECM deposition; while Cluster E has a lesion pattern more similar to ODAD, which is also non-specific. This may suggest that the transcriptomic profiles of each cluster differently influence the pattern and intensity of ECM deposition, resulting in distinct forms of fibrosis depending on the genes expressed.</p><p>In addition, the top 20 DGE highlighted upregulation of COL1A1 and CDH23 in CPF versus f-ILD (Figure S2C,D and Table S4); and downregulation of miR-663a in ODAD versus f-ILD, which directly targets transforming growth factor (TGF)-β1<span><sup>6</sup></span> (Figure S3C-D and Table S5). However, the WP Lung Fibrosis gene set (GSEA systematic name M39477) did not reveal DGE between the groups, reinforcing the similarity in the fibrotic pathway pattern (Figures S2E and S3E; Tables S6 and S7).</p><p>To ascertain the similarity in the gene expression levels of CPF and ODAD with f-ILD, we performed the DE analysis of each group against CTR-minimally altered pulmonary parenchyma with significantly lower collagen fibre deposition compared to the other groups (Table S1 and Figure 1J–M). A Venn diagram was generated from the DGE results (ODAD vs. CTR, CPF vs. CTR and f-ILD vs. CTR) to highlight the overlapping up and downregulated genes. As a result, 86 genes (71 upregulated, 15 downregulated) were commonly expressed in CPF and f-ILD (Table S8 and Figure 2). The distinctiveness of these genes lies in their absence from the ODAD group, suggesting transcription under chronic injury conditions without an active injurious stimulus, which might be considered as “fibrosis-related genes”. These genes likely play a pivotal role in sustaining fibrosis in a chronic and advanced state.</p><p>Indeed, the upregulated Fibrosis-related genes show significant enrichment in pathways related to WNT signalling (Figure 3A,B), suggesting a potential role in the progression of post-CPF, possibly by promoting fibrosis and epithelial-mesenchymal transition (EMT).<span><sup>7</sup></span> Additionally, the Cadherin signalling pathway (Figure 3B) is also significantly enriched, further supporting its involvement in EMTs. To confirm the gene expression findings (Figure S4A–D), we selected two genes from the group of 86, MUC5ac and WNT10a, both of which are already widely used in diagnostic immunohistochemistry (IHC). We observed higher expression of goblet cell hyperplasia MUC5ac+ in CPF and f-ILD compared to the other groups (Figure 3C,D, <i>p</i> < .05), as reported in other studies<span><sup>8</sup></span>; and higher in-situ presence of WNT10a+ in squamous cell metaplasia in CPF and f-ILD (Figure 3E,F, <i>p</i> < .05), consistent with its role in pulmonary fibrosis as described in other studies.<span><sup>7</sup></span></p><p>The Venn diagram also emphasized 31 genes (23 upregulated and eight downregulated) commonly expressed across the three groups (ODAD, CPF and f-ILD) (Table S9 and Figure 2). These genes likely contribute to the transition from the early fibrotic stage in ODAD to the more chronic fibrotic injury observed in CPF. Their continued presence in well-established fibrosis (f-ILD) underscores their importance in fibrosis progression, leading us to classify them as “progression-related genes.” The enrichment analysis of the upregulated genes from this list revealed a significant association with the transcription factors SMAD2 and SMAD3 (Figure 4A), which are central to TGF-β signalling, a key pathway in EMT and the advancement of fibrotic diseases, including post-CPF. Additionally, these genes showed a strong link to the “innate immunity evasion and cell-specific immune response” pathway associated with SARS-CoV-2 infections (Figure 4B). This pathway is crucial for understanding how the virus evades the host immune responses, potentially influencing the development of severe conditions like post-CPF by disrupting immune detection and altering cell cycle regulation.</p><p>To further validate the gene expression findings (Figure S4E–J), we selected two additional markers, KRT5 and MUC4, both widely used in diagnostic IHC. Increased in-situ expression of the epithelial marker KRT5+ in basal cell hyperplasia was observed in all groups compared to CTR (Figure 4C,D, <i>p</i> < .05) consistent with squamous metaplasia reported in COVID-19 cases.<span><sup>9</sup></span> Similarly, elevated in-situ MUC4+ expression in bronchial goblet cell hyperplasia (Figure 4E,F) was observed, consistent with findings in idiopathic pulmonary fibrosis (IPF).<span><sup>10</sup></span> The authors addressed MUC4 as part of the TGF-β1 canonical pathway, suggesting its role in the fibrotic microenvironment.</p><p>In conclusion, our study identifies a gene expression profile associated with COVID-19 progression to pulmonary fibrosis, revealing shared pathways with f-ILDs. In this way, the KRT5+ cells impair epithelial repair, while MUC4 overexpression exacerbates inflammation and tissue damage, restricting proper regeneration and promoting pulmonary fibrosis. MUC5AC maintains inflammation through mucus hypersecretion, and WNT10a drives fibroblast proliferation and ECM production. Continuous activation of the Wnt pathway by WNT10a contributes to tissue stiffness, which is crucial for sustaining pulmonary fibrosis. Furthermore, we demonstrate increased transcriptomic and in-situ expression of MUC4 and KRT5, suggesting their pivotal role in fibrosis progression and potential as early diagnostic biomarkers in transbronchial biopsy samples. However, a limitation of our study is that it captures gene expression at a single time-point, and longitudinal studies are needed to track gene expression changes from the acute infection phase to fibrosis development. Additionally, further validation of these biomarkers in larger cohorts, as well as investigation into their underlying mechanisms, is necessary given their significant potential for clinical practice as immunohistochemical markers for early intervention in fibrotic diseases.</p><p>Conceptualization: Sabrina Setembre Batah and Alexandre Todorovic Fabro; Formal analysis: Sabrina Setembre Batah, Amanda Piveta Schnepper, Robson Francisco Carvalho and João Paulo Facio Almeida; Funding acquisition: Sabrina Setembre Batah and Alexandre Todorovic Fabro; Investigation: Sabrina Setembre Batah, Juliana Rocha Souza Chiappetto, Tales Rubens de Nadai, Marcel Konigkam Santos, Li Siyuan Wada, Danilo Tadao Wada, Andrea Antunes Cetlin, Bruno Guedes Baldi and Suzana Tanni; Methodology: Sabrina Setembre Batah, Andrea Jazel Rodriguez-Herrera, Maria Júlia Faci do Marco, Juliana Rocha Souza Chiappetto, Mariana Gatto, Simone Alves do Vale, Robson Aparecido Prudente, Amanda Piveta Schnepper and João Paulo Facio Almeida; Project administration: Alexandre Todorovic Fabro; Resources: Robson Francisco Carvalho, José Baddini-Martinez, Bruno Guedes Baldi, Suzana Tanni and Alexandre Todorovic Fabro; Software: Sabrina Setembre Batah, Amanda Piveta Schnepper, Robson Francisco Carvalho and João Paulo Facio Almeida; Supervision: Vera Luiza Capelozzi, Rosane Duarte Achcar and Alexandre Todorovic Fabro; Validation: Sabrina Setembre Batah, Robson Francisco Carvalho and Alexandre Todorovic Fabro; Visualization: José Baddini-Martinez, Vera Luiza Capelozzi, Rosane Duarte Achcar and Alexandre Todorovic Fabro; Writing—original draft: Sabrina Setembre Batah and Alexandre Todorovic Fabro; Writing—review & editing: Sabrina Setembre Batah, Robson Francisco Carvalho, José Baddini-Martinez, Vera Luiza Capelozzi, Suzana Tanni, Rosane Duarte Achcar and Alexandre Todorovic Fabro.</p><p>The authors declare no conflict of interest.</p><p>This research was supported by São Paulo Research Foundation (Fapesp 22/02821-0; 20/13370-4; 23/10186-6; 23/04199-8; 21/09024-6; 23/10186-6; 23/04199-8; 23/10184-3) and by the National Council for Scientific and Technological Development (CNPq 310415/2021-7).</p><p>The Research Ethics Committee approved this study, and written informed consent was waived (CAAE: 43040920.0.0000.5440, 03737018.6.0000.5440 and 65315822.0.0000.5411).</p>","PeriodicalId":10189,"journal":{"name":"Clinical and Translational Medicine","volume":"14 11","pages":""},"PeriodicalIF":7.9000,"publicationDate":"2024-11-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11560857/pdf/","citationCount":"0","resultStr":"{\"title\":\"Transcriptomic profiling reveals the dynamics of fibrotic progression-related gene expression into post-coronavirus disease 2019 pulmonary fibrosis\",\"authors\":\"Sabrina Setembre Batah, Andrea Jazel Rodriguez-Herrera, Maria Júlia Faci do Marco, Juliana Rocha Souza Chiappetto, Mariana Gatto, Simone Alves do Vale, Robson Aparecido Prudente, Amanda Piveta Schnepper, Robson Francisco Carvalho, João Paulo Facio Almeida, Tales Rubens de Nadai, Marcel Konigkam Santos, Li Siyuan Wada, José Baddini-Martinez, Danilo Tadao Wada, Andrea Antunes Cetlin, Vera Luiza Capelozzi, Bruno Guedes Baldi, Suzana Tanni, Rosane Duarte Achcar, Alexandre Todorovic Fabro\",\"doi\":\"10.1002/ctm2.70088\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Dear Editor,</p><p>Our study has identified a gene expression profile associated with the progression of coronavirus disease 2019 (COVID-19) to pulmonary fibrosis in a pro-fibrotic environment similar to that found in fibrosing interstitial lung diseases (f-ILDs). Briefly, we noted the common expression of 86 genes in post-COVID-19 pulmonary fibrosis (post-CPF) and f-ILDs, indicating their likely involvement in perpetuating pulmonary fibrosis through shared fibrotic pathways—confirmed by the in-situ expression of MUC5ac and WNT10a. Furthermore, an additional set of 31 genes exhibited common expression patterns between subacute COVID-19, the so-called organizing diffuse alveolar damage (ODAD), and CPF, as well as f-ILDs. Among those genes, MUC4 and KRT5 were confirmed by immunohistochemistry, suggesting their role as potential predictors for the early outcome of possible pulmonary fibrosis.</p><p>Post-CPF is a long-term complication diagnosed by clinical setting, pulmonary function tests and/or image examinations.<span><sup>1</sup></span> Initially, some COVID-19-infected patients develop acute respiratory distress syndrome (ARDS) during the exudative phase of DAD, marked by cytokine storm and immune cell recruitment.<span><sup>2</sup></span> Following the inflammatory peak and pneumocyte injury, myofibroblast activation triggers extracellular matrix (ECM) deposition, leading to ODAD-phase which typically restores to typical lung architecture. However, some patients progress to pulmonary fibrosis<span><sup>3</sup></span> with morphological changes that are driven by a complex pathophysiological sequence and dynamic gene expression shifts. In the end, the fibrotic outcome can resemble other f-ILDs. Identifying gene expression levels linked to the progression from ODAD to CPF is crucial for finding biomarkers for early diagnosis. Our study aimed to identify potential biomarkers in gene expression associated with fibrotic progression to CPF by analyzing the transcriptome of patients with ODAD, CPF, f-ILDs and controls.</p><p>As previously described by Batah et al.,<span><sup>4</sup></span> autopsies from the ODAD group revealed ODAD-phase with bronchiolar metaplasia, myxoid fibrosis, myofibroblastic activation and extensive alveolar septal thickening with collagen types I and III deposition (Table S1; Figure 1A–C). Meanwhile, after an average of 324.6 days following the initial positive nasopharyngeal swab for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), patients from the CPF group developed pulmonary fibrosis with bronchiolar metaplasia and parenchymal remodelling with increased collagen deposition, especially type I (suppinfo1; Figure 1D–F). Although the common remodelling profile, the differential gene expression (DGE) analysis between ODAD and CPF revealed distinct gene signatures (Figure S1A,B), Some of the top 20 DGEs reflect the manifestation of ARDS in ODAD patients (Figure S1C,D and Table S2). For example, the upregulation of SERPINE1 -fibrinolysis inhibitor- in ODAD suggests the accumulation of deposited fibrin as a better pathophysiological response to SARS-CoV-2.<span><sup>5</sup></span> However, as mentioned earlier, both groups revealed parenchymal remodelling, and the WP Lung Fibrosis gene set (GSEA systematic name M39477) highlighted only a few DGE between the groups: upregulated MMP9 and TERT and downregulated MUC5B and FGF1 in ODAD compared to CPF (Figure S1E and Table S3). Therefore, some fibrotic pathways might be present in both groups, suggesting a possible similarity with the transcriptomic profile of f-ILD patients.</p><p>In fact, our data revealed a significant similarity in gene expression among the groups compared to f-ILD, presenting dense fibrosis, architectural distortion, bronchiolar metaplasia, fibroblast foci and collagen types I and III deposition (Table S1 and Figure 1G–I). The similarity is seen by the overlap of cases in the paired DGE analyses between CPF versus f-ILD (Figure S2A,B) and ODAD versus f-ILD (Figure S3A,B). In both principal component analyses, f-ILD patients were divided into two distinct clusters: In Figure S2A, Cluster A is distinct from the other cases, while Cluster B is found among the CPF patients. Cluster A displays a bronchiolocentric remodelling pattern, whereas Cluster B exhibits a non-specific lesion pattern characterized by uniform thickening of the pulmonary interstitium, similar to that observed in CPF patients. Similarly, in Figure S3A, Cluster D has the same patients as Cluster A, who also exhibit bronchiolocentric ECM deposition; while Cluster E has a lesion pattern more similar to ODAD, which is also non-specific. This may suggest that the transcriptomic profiles of each cluster differently influence the pattern and intensity of ECM deposition, resulting in distinct forms of fibrosis depending on the genes expressed.</p><p>In addition, the top 20 DGE highlighted upregulation of COL1A1 and CDH23 in CPF versus f-ILD (Figure S2C,D and Table S4); and downregulation of miR-663a in ODAD versus f-ILD, which directly targets transforming growth factor (TGF)-β1<span><sup>6</sup></span> (Figure S3C-D and Table S5). However, the WP Lung Fibrosis gene set (GSEA systematic name M39477) did not reveal DGE between the groups, reinforcing the similarity in the fibrotic pathway pattern (Figures S2E and S3E; Tables S6 and S7).</p><p>To ascertain the similarity in the gene expression levels of CPF and ODAD with f-ILD, we performed the DE analysis of each group against CTR-minimally altered pulmonary parenchyma with significantly lower collagen fibre deposition compared to the other groups (Table S1 and Figure 1J–M). A Venn diagram was generated from the DGE results (ODAD vs. CTR, CPF vs. CTR and f-ILD vs. CTR) to highlight the overlapping up and downregulated genes. As a result, 86 genes (71 upregulated, 15 downregulated) were commonly expressed in CPF and f-ILD (Table S8 and Figure 2). The distinctiveness of these genes lies in their absence from the ODAD group, suggesting transcription under chronic injury conditions without an active injurious stimulus, which might be considered as “fibrosis-related genes”. These genes likely play a pivotal role in sustaining fibrosis in a chronic and advanced state.</p><p>Indeed, the upregulated Fibrosis-related genes show significant enrichment in pathways related to WNT signalling (Figure 3A,B), suggesting a potential role in the progression of post-CPF, possibly by promoting fibrosis and epithelial-mesenchymal transition (EMT).<span><sup>7</sup></span> Additionally, the Cadherin signalling pathway (Figure 3B) is also significantly enriched, further supporting its involvement in EMTs. To confirm the gene expression findings (Figure S4A–D), we selected two genes from the group of 86, MUC5ac and WNT10a, both of which are already widely used in diagnostic immunohistochemistry (IHC). We observed higher expression of goblet cell hyperplasia MUC5ac+ in CPF and f-ILD compared to the other groups (Figure 3C,D, <i>p</i> < .05), as reported in other studies<span><sup>8</sup></span>; and higher in-situ presence of WNT10a+ in squamous cell metaplasia in CPF and f-ILD (Figure 3E,F, <i>p</i> < .05), consistent with its role in pulmonary fibrosis as described in other studies.<span><sup>7</sup></span></p><p>The Venn diagram also emphasized 31 genes (23 upregulated and eight downregulated) commonly expressed across the three groups (ODAD, CPF and f-ILD) (Table S9 and Figure 2). These genes likely contribute to the transition from the early fibrotic stage in ODAD to the more chronic fibrotic injury observed in CPF. Their continued presence in well-established fibrosis (f-ILD) underscores their importance in fibrosis progression, leading us to classify them as “progression-related genes.” The enrichment analysis of the upregulated genes from this list revealed a significant association with the transcription factors SMAD2 and SMAD3 (Figure 4A), which are central to TGF-β signalling, a key pathway in EMT and the advancement of fibrotic diseases, including post-CPF. Additionally, these genes showed a strong link to the “innate immunity evasion and cell-specific immune response” pathway associated with SARS-CoV-2 infections (Figure 4B). This pathway is crucial for understanding how the virus evades the host immune responses, potentially influencing the development of severe conditions like post-CPF by disrupting immune detection and altering cell cycle regulation.</p><p>To further validate the gene expression findings (Figure S4E–J), we selected two additional markers, KRT5 and MUC4, both widely used in diagnostic IHC. Increased in-situ expression of the epithelial marker KRT5+ in basal cell hyperplasia was observed in all groups compared to CTR (Figure 4C,D, <i>p</i> < .05) consistent with squamous metaplasia reported in COVID-19 cases.<span><sup>9</sup></span> Similarly, elevated in-situ MUC4+ expression in bronchial goblet cell hyperplasia (Figure 4E,F) was observed, consistent with findings in idiopathic pulmonary fibrosis (IPF).<span><sup>10</sup></span> The authors addressed MUC4 as part of the TGF-β1 canonical pathway, suggesting its role in the fibrotic microenvironment.</p><p>In conclusion, our study identifies a gene expression profile associated with COVID-19 progression to pulmonary fibrosis, revealing shared pathways with f-ILDs. In this way, the KRT5+ cells impair epithelial repair, while MUC4 overexpression exacerbates inflammation and tissue damage, restricting proper regeneration and promoting pulmonary fibrosis. MUC5AC maintains inflammation through mucus hypersecretion, and WNT10a drives fibroblast proliferation and ECM production. Continuous activation of the Wnt pathway by WNT10a contributes to tissue stiffness, which is crucial for sustaining pulmonary fibrosis. Furthermore, we demonstrate increased transcriptomic and in-situ expression of MUC4 and KRT5, suggesting their pivotal role in fibrosis progression and potential as early diagnostic biomarkers in transbronchial biopsy samples. However, a limitation of our study is that it captures gene expression at a single time-point, and longitudinal studies are needed to track gene expression changes from the acute infection phase to fibrosis development. Additionally, further validation of these biomarkers in larger cohorts, as well as investigation into their underlying mechanisms, is necessary given their significant potential for clinical practice as immunohistochemical markers for early intervention in fibrotic diseases.</p><p>Conceptualization: Sabrina Setembre Batah and Alexandre Todorovic Fabro; Formal analysis: Sabrina Setembre Batah, Amanda Piveta Schnepper, Robson Francisco Carvalho and João Paulo Facio Almeida; Funding acquisition: Sabrina Setembre Batah and Alexandre Todorovic Fabro; Investigation: Sabrina Setembre Batah, Juliana Rocha Souza Chiappetto, Tales Rubens de Nadai, Marcel Konigkam Santos, Li Siyuan Wada, Danilo Tadao Wada, Andrea Antunes Cetlin, Bruno Guedes Baldi and Suzana Tanni; Methodology: Sabrina Setembre Batah, Andrea Jazel Rodriguez-Herrera, Maria Júlia Faci do Marco, Juliana Rocha Souza Chiappetto, Mariana Gatto, Simone Alves do Vale, Robson Aparecido Prudente, Amanda Piveta Schnepper and João Paulo Facio Almeida; Project administration: Alexandre Todorovic Fabro; Resources: Robson Francisco Carvalho, José Baddini-Martinez, Bruno Guedes Baldi, Suzana Tanni and Alexandre Todorovic Fabro; Software: Sabrina Setembre Batah, Amanda Piveta Schnepper, Robson Francisco Carvalho and João Paulo Facio Almeida; Supervision: Vera Luiza Capelozzi, Rosane Duarte Achcar and Alexandre Todorovic Fabro; Validation: Sabrina Setembre Batah, Robson Francisco Carvalho and Alexandre Todorovic Fabro; Visualization: José Baddini-Martinez, Vera Luiza Capelozzi, Rosane Duarte Achcar and Alexandre Todorovic Fabro; Writing—original draft: Sabrina Setembre Batah and Alexandre Todorovic Fabro; Writing—review & editing: Sabrina Setembre Batah, Robson Francisco Carvalho, José Baddini-Martinez, Vera Luiza Capelozzi, Suzana Tanni, Rosane Duarte Achcar and Alexandre Todorovic Fabro.</p><p>The authors declare no conflict of interest.</p><p>This research was supported by São Paulo Research Foundation (Fapesp 22/02821-0; 20/13370-4; 23/10186-6; 23/04199-8; 21/09024-6; 23/10186-6; 23/04199-8; 23/10184-3) and by the National Council for Scientific and Technological Development (CNPq 310415/2021-7).</p><p>The Research Ethics Committee approved this study, and written informed consent was waived (CAAE: 43040920.0.0000.5440, 03737018.6.0000.5440 and 65315822.0.0000.5411).</p>\",\"PeriodicalId\":10189,\"journal\":{\"name\":\"Clinical and Translational Medicine\",\"volume\":\"14 11\",\"pages\":\"\"},\"PeriodicalIF\":7.9000,\"publicationDate\":\"2024-11-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11560857/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Translational Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ctm2.70088\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ctm2.70088","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
摘要
亲爱的编辑,我们的研究发现了与2019年冠状病毒病(COVID-19)进展为肺纤维化相关的基因表达谱,这种肺纤维化的促纤维化环境类似于纤维化间质性肺病(f-ILDs)。简而言之,我们注意到在 COVID-19 后肺纤维化(post-CPF)和 f-ILDs 中有 86 个基因的共同表达,这表明它们可能通过共同的纤维化途径参与了肺纤维化的延续--MUC5ac 和 WNT10a 的原位表达证实了这一点。此外,还有一组 31 个基因在亚急性 COVID-19、所谓的组织弥漫性肺泡损伤(ODAD)和 CPF 以及 f-ILD 之间表现出共同的表达模式。在这些基因中,MUC4 和 KRT5 通过免疫组化得到了证实,表明它们可能是肺纤维化早期结果的潜在预测因子。最初,一些 COVID-19 感染者会在 DAD 的渗出期出现急性呼吸窘迫综合征(ARDS),细胞因子风暴和免疫细胞募集是其特征。2 炎症高峰和肺细胞损伤之后,肌成纤维细胞活化引发细胞外基质(ECM)沉积,导致 ODAD 阶段,该阶段通常会恢复典型的肺结构。然而,有些患者会发展为肺纤维化3,其形态学变化是由复杂的病理生理顺序和动态基因表达变化驱动的。最终,纤维化的结果可能与其他 f-ILD 相似。确定与 ODAD 向 CPF 进展相关的基因表达水平,对于找到早期诊断的生物标志物至关重要。我们的研究旨在通过分析 ODAD、CPF、f-ILDs 患者和对照组的转录组,找出与纤维化进展至 CPF 相关的潜在基因表达生物标志物。正如 Batah 等人先前所描述的那样,4 ODAD 组的尸检结果显示,ODAD 期患者出现支气管化生、肌样纤维化、肌成纤维细胞活化和广泛的肺泡间隔增厚,并伴有 I 型和 III 型胶原沉积(表 S1;图 1A-C)。同时,在鼻咽拭子检测严重急性呼吸系统综合征冠状病毒 2(SARS-CoV-2)初次阳性后平均 324.6 天,CPF 组患者出现肺纤维化,支气管化生和实质重塑,胶原沉积增加,尤其是 I 型胶原(suppinfo1;图 1D-F)。虽然ODAD和CPF的重塑特征相同,但其差异基因表达(DGE)分析却显示出不同的基因特征(图S1A,B),前20个DGE中的一些反映了ODAD患者ARDS的表现(图S1C,D和表S2)。例如,ODAD 中纤维蛋白溶解抑制因子 SERPINE1 的上调表明,沉积的纤维蛋白的积累是对 SARS-CoV-2 的更好的病理生理反应。5 然而,如前所述,两组均显示出肺实质重塑,WP 肺纤维化基因组(GSEA 系统名称 M39477)仅强调了两组之间的一些 DGE:与 CPF 相比,ODAD 中 MMP9 和 TERT 上调,MUC5B 和 FGF1 下调(图 S1E 和表 S3)。事实上,我们的数据显示,与 f-ILD 相比,各组间的基因表达具有显著的相似性,均表现为致密纤维化、结构扭曲、支气管化生、成纤维细胞灶以及 I 型和 III 型胶原沉积(表 S1 和图 1G-I)。CPF 与 f-ILD 的配对 DGE 分析(图 S2A,B)和 ODAD 与 f-ILD 的配对 DGE 分析(图 S3A,B)中的病例重叠可以看出这种相似性。在这两项主成分分析中,f-ILD 患者被分为两个不同的群组:在图 S2A 中,簇 A 与其他病例截然不同,而簇 B 则出现在 CPF 患者中。簇 A 显示出以支气管为中心的重塑模式,而簇 B 则显示出以肺间质均匀增厚为特征的非特异性病变模式,与 CPF 患者中观察到的病变模式相似。同样,在图 S3A 中,群组 D 的患者与群组 A 相同,也表现出以支气管为中心的 ECM 沉积;而群组 E 的病变模式更类似于 ODAD,也是非特异性的。这可能表明,每个群组的转录组特征会对 ECM 沉积的模式和强度产生不同的影响,从而导致不同形式的纤维化,具体取决于所表达的基因。 然而,我们研究的局限性在于它捕捉的是单个时间点的基因表达,因此需要进行纵向研究来追踪从急性感染阶段到纤维化发展阶段的基因表达变化。此外,鉴于这些生物标志物作为早期干预纤维化疾病的免疫组化标志物在临床实践中的巨大潜力,有必要在更大的群体中进一步验证这些生物标志物,并研究其潜在机制:Sabrina Setembre Batah 和 Alexandre Todorovic Fabro;形式分析:Sabrina Setembre Batah、Amanda Piveta Schnepper、Robson Francisco Carvalho 和 João Paulo Facio Almeida;资金获取:Sabrina Setembre Batah 和 Alexandre Todorovic Fabro;调查:Sabrina Setembre Batah、Juliana Rocha Souza Chiappetto、Tales Rubens de Nadai、Marcel Konigkam Santos、Li Siyuan Wada、Danilo Tadao Wada、Andrea Antunes Cetlin、Bruno Guedes Baldi 和 Suzana Tanni;方法:Sabrina Setembre Batah、Andrea Jazel Rodriguez-Herrera、Maria Júlia Faci do Marco、Juliana Rocha Souza Chiappetto、Mariana Gatto、Simone Alves do Vale、Robson Aparecido Prudente、Amanda Piveta Schnepper 和 João Paulo Facio Almeida;项目管理:Alexandre Todorovic Fabro;资源:Robson Francisco Carvalho、José Baddini-Martinez、Bruno Guedes Baldi、Suzana Tanni 和 Alexandre Todorovic Fabro;软件:Sabrina Setembre Batah、Amanda Piveta Schnepper、Robson Francisco Carvalho 和 João Paulo Facio Almeida;监督:Vera Luiza Capelozzi、Rosane Duarte Achcar 和 Alexandre Todorovic Fabro;验证:Sabrina Setembre Batah、Robson Francisco Carvalho 和 Alexandre Todorovic Fabro;可视化:José Baddini-Martinez, Vera Luiza Capelozzi, Rosane Duarte Achcar 和 Alexandre Todorovic Fabro;写作-原稿:Sabrina Setembre Batah 和 Alexandre Todorovic Fabro;撰写-审阅;编辑:Sabrina Setembre Batah、Robson Francisco Carvalho、José Baddini-Martinez、Vera Luiza Capelozzi、Suzana Tanni、Rosane Duarte Achcar 和 Alexandre Todorovic Fabro。作者声明无利益冲突。本研究得到了圣保罗研究基金会(Fapesp 22/02821-0; 20/13370-4; 23/10186-6; 23/04199-8; 21/09024-6; 23/10186-6; 23/04199-8; 23/10184-3)和国家科技发展委员会(CNPq 310415/2021-7)的支持。研究伦理委员会批准了这项研究,并免除了知情同意书(CAAE:43040920.0.0000.5440、03737018.6.0000.5440 和 65315822.0.0000.5411)。
Transcriptomic profiling reveals the dynamics of fibrotic progression-related gene expression into post-coronavirus disease 2019 pulmonary fibrosis
Dear Editor,
Our study has identified a gene expression profile associated with the progression of coronavirus disease 2019 (COVID-19) to pulmonary fibrosis in a pro-fibrotic environment similar to that found in fibrosing interstitial lung diseases (f-ILDs). Briefly, we noted the common expression of 86 genes in post-COVID-19 pulmonary fibrosis (post-CPF) and f-ILDs, indicating their likely involvement in perpetuating pulmonary fibrosis through shared fibrotic pathways—confirmed by the in-situ expression of MUC5ac and WNT10a. Furthermore, an additional set of 31 genes exhibited common expression patterns between subacute COVID-19, the so-called organizing diffuse alveolar damage (ODAD), and CPF, as well as f-ILDs. Among those genes, MUC4 and KRT5 were confirmed by immunohistochemistry, suggesting their role as potential predictors for the early outcome of possible pulmonary fibrosis.
Post-CPF is a long-term complication diagnosed by clinical setting, pulmonary function tests and/or image examinations.1 Initially, some COVID-19-infected patients develop acute respiratory distress syndrome (ARDS) during the exudative phase of DAD, marked by cytokine storm and immune cell recruitment.2 Following the inflammatory peak and pneumocyte injury, myofibroblast activation triggers extracellular matrix (ECM) deposition, leading to ODAD-phase which typically restores to typical lung architecture. However, some patients progress to pulmonary fibrosis3 with morphological changes that are driven by a complex pathophysiological sequence and dynamic gene expression shifts. In the end, the fibrotic outcome can resemble other f-ILDs. Identifying gene expression levels linked to the progression from ODAD to CPF is crucial for finding biomarkers for early diagnosis. Our study aimed to identify potential biomarkers in gene expression associated with fibrotic progression to CPF by analyzing the transcriptome of patients with ODAD, CPF, f-ILDs and controls.
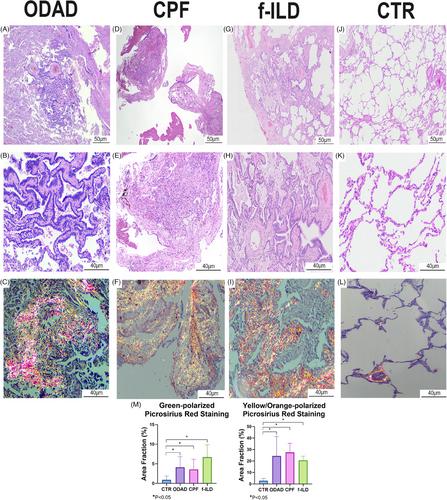
As previously described by Batah et al.,4 autopsies from the ODAD group revealed ODAD-phase with bronchiolar metaplasia, myxoid fibrosis, myofibroblastic activation and extensive alveolar septal thickening with collagen types I and III deposition (Table S1; Figure 1A–C). Meanwhile, after an average of 324.6 days following the initial positive nasopharyngeal swab for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), patients from the CPF group developed pulmonary fibrosis with bronchiolar metaplasia and parenchymal remodelling with increased collagen deposition, especially type I (suppinfo1; Figure 1D–F). Although the common remodelling profile, the differential gene expression (DGE) analysis between ODAD and CPF revealed distinct gene signatures (Figure S1A,B), Some of the top 20 DGEs reflect the manifestation of ARDS in ODAD patients (Figure S1C,D and Table S2). For example, the upregulation of SERPINE1 -fibrinolysis inhibitor- in ODAD suggests the accumulation of deposited fibrin as a better pathophysiological response to SARS-CoV-2.5 However, as mentioned earlier, both groups revealed parenchymal remodelling, and the WP Lung Fibrosis gene set (GSEA systematic name M39477) highlighted only a few DGE between the groups: upregulated MMP9 and TERT and downregulated MUC5B and FGF1 in ODAD compared to CPF (Figure S1E and Table S3). Therefore, some fibrotic pathways might be present in both groups, suggesting a possible similarity with the transcriptomic profile of f-ILD patients.
In fact, our data revealed a significant similarity in gene expression among the groups compared to f-ILD, presenting dense fibrosis, architectural distortion, bronchiolar metaplasia, fibroblast foci and collagen types I and III deposition (Table S1 and Figure 1G–I). The similarity is seen by the overlap of cases in the paired DGE analyses between CPF versus f-ILD (Figure S2A,B) and ODAD versus f-ILD (Figure S3A,B). In both principal component analyses, f-ILD patients were divided into two distinct clusters: In Figure S2A, Cluster A is distinct from the other cases, while Cluster B is found among the CPF patients. Cluster A displays a bronchiolocentric remodelling pattern, whereas Cluster B exhibits a non-specific lesion pattern characterized by uniform thickening of the pulmonary interstitium, similar to that observed in CPF patients. Similarly, in Figure S3A, Cluster D has the same patients as Cluster A, who also exhibit bronchiolocentric ECM deposition; while Cluster E has a lesion pattern more similar to ODAD, which is also non-specific. This may suggest that the transcriptomic profiles of each cluster differently influence the pattern and intensity of ECM deposition, resulting in distinct forms of fibrosis depending on the genes expressed.
In addition, the top 20 DGE highlighted upregulation of COL1A1 and CDH23 in CPF versus f-ILD (Figure S2C,D and Table S4); and downregulation of miR-663a in ODAD versus f-ILD, which directly targets transforming growth factor (TGF)-β16 (Figure S3C-D and Table S5). However, the WP Lung Fibrosis gene set (GSEA systematic name M39477) did not reveal DGE between the groups, reinforcing the similarity in the fibrotic pathway pattern (Figures S2E and S3E; Tables S6 and S7).
To ascertain the similarity in the gene expression levels of CPF and ODAD with f-ILD, we performed the DE analysis of each group against CTR-minimally altered pulmonary parenchyma with significantly lower collagen fibre deposition compared to the other groups (Table S1 and Figure 1J–M). A Venn diagram was generated from the DGE results (ODAD vs. CTR, CPF vs. CTR and f-ILD vs. CTR) to highlight the overlapping up and downregulated genes. As a result, 86 genes (71 upregulated, 15 downregulated) were commonly expressed in CPF and f-ILD (Table S8 and Figure 2). The distinctiveness of these genes lies in their absence from the ODAD group, suggesting transcription under chronic injury conditions without an active injurious stimulus, which might be considered as “fibrosis-related genes”. These genes likely play a pivotal role in sustaining fibrosis in a chronic and advanced state.
Indeed, the upregulated Fibrosis-related genes show significant enrichment in pathways related to WNT signalling (Figure 3A,B), suggesting a potential role in the progression of post-CPF, possibly by promoting fibrosis and epithelial-mesenchymal transition (EMT).7 Additionally, the Cadherin signalling pathway (Figure 3B) is also significantly enriched, further supporting its involvement in EMTs. To confirm the gene expression findings (Figure S4A–D), we selected two genes from the group of 86, MUC5ac and WNT10a, both of which are already widely used in diagnostic immunohistochemistry (IHC). We observed higher expression of goblet cell hyperplasia MUC5ac+ in CPF and f-ILD compared to the other groups (Figure 3C,D, p < .05), as reported in other studies8; and higher in-situ presence of WNT10a+ in squamous cell metaplasia in CPF and f-ILD (Figure 3E,F, p < .05), consistent with its role in pulmonary fibrosis as described in other studies.7
The Venn diagram also emphasized 31 genes (23 upregulated and eight downregulated) commonly expressed across the three groups (ODAD, CPF and f-ILD) (Table S9 and Figure 2). These genes likely contribute to the transition from the early fibrotic stage in ODAD to the more chronic fibrotic injury observed in CPF. Their continued presence in well-established fibrosis (f-ILD) underscores their importance in fibrosis progression, leading us to classify them as “progression-related genes.” The enrichment analysis of the upregulated genes from this list revealed a significant association with the transcription factors SMAD2 and SMAD3 (Figure 4A), which are central to TGF-β signalling, a key pathway in EMT and the advancement of fibrotic diseases, including post-CPF. Additionally, these genes showed a strong link to the “innate immunity evasion and cell-specific immune response” pathway associated with SARS-CoV-2 infections (Figure 4B). This pathway is crucial for understanding how the virus evades the host immune responses, potentially influencing the development of severe conditions like post-CPF by disrupting immune detection and altering cell cycle regulation.
To further validate the gene expression findings (Figure S4E–J), we selected two additional markers, KRT5 and MUC4, both widely used in diagnostic IHC. Increased in-situ expression of the epithelial marker KRT5+ in basal cell hyperplasia was observed in all groups compared to CTR (Figure 4C,D, p < .05) consistent with squamous metaplasia reported in COVID-19 cases.9 Similarly, elevated in-situ MUC4+ expression in bronchial goblet cell hyperplasia (Figure 4E,F) was observed, consistent with findings in idiopathic pulmonary fibrosis (IPF).10 The authors addressed MUC4 as part of the TGF-β1 canonical pathway, suggesting its role in the fibrotic microenvironment.
In conclusion, our study identifies a gene expression profile associated with COVID-19 progression to pulmonary fibrosis, revealing shared pathways with f-ILDs. In this way, the KRT5+ cells impair epithelial repair, while MUC4 overexpression exacerbates inflammation and tissue damage, restricting proper regeneration and promoting pulmonary fibrosis. MUC5AC maintains inflammation through mucus hypersecretion, and WNT10a drives fibroblast proliferation and ECM production. Continuous activation of the Wnt pathway by WNT10a contributes to tissue stiffness, which is crucial for sustaining pulmonary fibrosis. Furthermore, we demonstrate increased transcriptomic and in-situ expression of MUC4 and KRT5, suggesting their pivotal role in fibrosis progression and potential as early diagnostic biomarkers in transbronchial biopsy samples. However, a limitation of our study is that it captures gene expression at a single time-point, and longitudinal studies are needed to track gene expression changes from the acute infection phase to fibrosis development. Additionally, further validation of these biomarkers in larger cohorts, as well as investigation into their underlying mechanisms, is necessary given their significant potential for clinical practice as immunohistochemical markers for early intervention in fibrotic diseases.
Conceptualization: Sabrina Setembre Batah and Alexandre Todorovic Fabro; Formal analysis: Sabrina Setembre Batah, Amanda Piveta Schnepper, Robson Francisco Carvalho and João Paulo Facio Almeida; Funding acquisition: Sabrina Setembre Batah and Alexandre Todorovic Fabro; Investigation: Sabrina Setembre Batah, Juliana Rocha Souza Chiappetto, Tales Rubens de Nadai, Marcel Konigkam Santos, Li Siyuan Wada, Danilo Tadao Wada, Andrea Antunes Cetlin, Bruno Guedes Baldi and Suzana Tanni; Methodology: Sabrina Setembre Batah, Andrea Jazel Rodriguez-Herrera, Maria Júlia Faci do Marco, Juliana Rocha Souza Chiappetto, Mariana Gatto, Simone Alves do Vale, Robson Aparecido Prudente, Amanda Piveta Schnepper and João Paulo Facio Almeida; Project administration: Alexandre Todorovic Fabro; Resources: Robson Francisco Carvalho, José Baddini-Martinez, Bruno Guedes Baldi, Suzana Tanni and Alexandre Todorovic Fabro; Software: Sabrina Setembre Batah, Amanda Piveta Schnepper, Robson Francisco Carvalho and João Paulo Facio Almeida; Supervision: Vera Luiza Capelozzi, Rosane Duarte Achcar and Alexandre Todorovic Fabro; Validation: Sabrina Setembre Batah, Robson Francisco Carvalho and Alexandre Todorovic Fabro; Visualization: José Baddini-Martinez, Vera Luiza Capelozzi, Rosane Duarte Achcar and Alexandre Todorovic Fabro; Writing—original draft: Sabrina Setembre Batah and Alexandre Todorovic Fabro; Writing—review & editing: Sabrina Setembre Batah, Robson Francisco Carvalho, José Baddini-Martinez, Vera Luiza Capelozzi, Suzana Tanni, Rosane Duarte Achcar and Alexandre Todorovic Fabro.
The authors declare no conflict of interest.
This research was supported by São Paulo Research Foundation (Fapesp 22/02821-0; 20/13370-4; 23/10186-6; 23/04199-8; 21/09024-6; 23/10186-6; 23/04199-8; 23/10184-3) and by the National Council for Scientific and Technological Development (CNPq 310415/2021-7).
The Research Ethics Committee approved this study, and written informed consent was waived (CAAE: 43040920.0.0000.5440, 03737018.6.0000.5440 and 65315822.0.0000.5411).
期刊介绍:
Clinical and Translational Medicine (CTM) is an international, peer-reviewed, open-access journal dedicated to accelerating the translation of preclinical research into clinical applications and fostering communication between basic and clinical scientists. It highlights the clinical potential and application of various fields including biotechnologies, biomaterials, bioengineering, biomarkers, molecular medicine, omics science, bioinformatics, immunology, molecular imaging, drug discovery, regulation, and health policy. With a focus on the bench-to-bedside approach, CTM prioritizes studies and clinical observations that generate hypotheses relevant to patients and diseases, guiding investigations in cellular and molecular medicine. The journal encourages submissions from clinicians, researchers, policymakers, and industry professionals.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


