Hangyul Cho, Taehoon Kim, Younsuk Lee, Dawoon Kim, Hansu Bae
{"title":"自发性脑内出血后最初 24 小时的总体血压变化和相关血压变化与死亡率:一项对 1,036 名患者进行的回顾性研究。","authors":"Hangyul Cho, Taehoon Kim, Younsuk Lee, Dawoon Kim, Hansu Bae","doi":"10.17085/apm.24039","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study aims to establish the individual contributions of blood pressure variability (BPV) indexes, categorized into overall and linked variability, to mortality following intracerebral hemorrhage (ICH) by examining the risk factors.</p><p><strong>Methods: </strong>Patients with spontaneous ICH (n = 1,036) were identified with valid blood pressures (BP) from the first 24-h systolic BP records in the Medical Information Mart for Intensive Care IV version 2.2 database (MIMIC IV). Information on the baseline characteristics, including age, sex, initial Glasgow Coma Scale (GCS) and National Institutes of Health Stroke Scale (NIHSS) scores, ICH location, Charlson comorbidity index score, and presence of diabetes with or without complications, were collected. Three indexes of BPV-range, standard deviation (SD), and generalized BPV (GBPV)-were calculated using the first 24-h systolic BPs. An automated stepwise variable-selection procedure was used to develop the final logistic model for predicting in-hospital mortality.</p><p><strong>Results: </strong>Out of 1,036 patients, 802 (77.4%) survived and were discharged after spontaneous ICH. Factors associated with mortality included age; male sex; ICH in the brainstem, ventricle, or multiple locations; low GCS score (< 9); high NIHSS score (> 20); and diabetes with complications. Mean systolic BP, SD, and GBPV were also linked to mortality. Higher GBPV notably increased the risk of in-hospital death, with an odds ratio of 3.21 (95% confidence interval, 2.10 to 4.97) for every + 10 mmHg/h change in GBPV.</p><p><strong>Conclusions: </strong>This study underscores the additional impact of GBPV, herein linked to BPV, on mortality following ICH, providing further insights into the management of blood pressure in the early stages of ICH treatment.</p>","PeriodicalId":101360,"journal":{"name":"Anesthesia and pain medicine","volume":"19 4","pages":"302-309"},"PeriodicalIF":3.2000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11558055/pdf/","citationCount":"0","resultStr":"{\"title\":\"Overall and linked blood pressure variabilities in the first 24 hours and mortality after spontaneous intracerebral hemorrhage: a retrospective study of 1,036 patients.\",\"authors\":\"Hangyul Cho, Taehoon Kim, Younsuk Lee, Dawoon Kim, Hansu Bae\",\"doi\":\"10.17085/apm.24039\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This study aims to establish the individual contributions of blood pressure variability (BPV) indexes, categorized into overall and linked variability, to mortality following intracerebral hemorrhage (ICH) by examining the risk factors.</p><p><strong>Methods: </strong>Patients with spontaneous ICH (n = 1,036) were identified with valid blood pressures (BP) from the first 24-h systolic BP records in the Medical Information Mart for Intensive Care IV version 2.2 database (MIMIC IV). Information on the baseline characteristics, including age, sex, initial Glasgow Coma Scale (GCS) and National Institutes of Health Stroke Scale (NIHSS) scores, ICH location, Charlson comorbidity index score, and presence of diabetes with or without complications, were collected. Three indexes of BPV-range, standard deviation (SD), and generalized BPV (GBPV)-were calculated using the first 24-h systolic BPs. An automated stepwise variable-selection procedure was used to develop the final logistic model for predicting in-hospital mortality.</p><p><strong>Results: </strong>Out of 1,036 patients, 802 (77.4%) survived and were discharged after spontaneous ICH. Factors associated with mortality included age; male sex; ICH in the brainstem, ventricle, or multiple locations; low GCS score (< 9); high NIHSS score (> 20); and diabetes with complications. Mean systolic BP, SD, and GBPV were also linked to mortality. Higher GBPV notably increased the risk of in-hospital death, with an odds ratio of 3.21 (95% confidence interval, 2.10 to 4.97) for every + 10 mmHg/h change in GBPV.</p><p><strong>Conclusions: </strong>This study underscores the additional impact of GBPV, herein linked to BPV, on mortality following ICH, providing further insights into the management of blood pressure in the early stages of ICH treatment.</p>\",\"PeriodicalId\":101360,\"journal\":{\"name\":\"Anesthesia and pain medicine\",\"volume\":\"19 4\",\"pages\":\"302-309\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11558055/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anesthesia and pain medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.17085/apm.24039\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/31 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia and pain medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17085/apm.24039","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Overall and linked blood pressure variabilities in the first 24 hours and mortality after spontaneous intracerebral hemorrhage: a retrospective study of 1,036 patients.
Background: This study aims to establish the individual contributions of blood pressure variability (BPV) indexes, categorized into overall and linked variability, to mortality following intracerebral hemorrhage (ICH) by examining the risk factors.
Methods: Patients with spontaneous ICH (n = 1,036) were identified with valid blood pressures (BP) from the first 24-h systolic BP records in the Medical Information Mart for Intensive Care IV version 2.2 database (MIMIC IV). Information on the baseline characteristics, including age, sex, initial Glasgow Coma Scale (GCS) and National Institutes of Health Stroke Scale (NIHSS) scores, ICH location, Charlson comorbidity index score, and presence of diabetes with or without complications, were collected. Three indexes of BPV-range, standard deviation (SD), and generalized BPV (GBPV)-were calculated using the first 24-h systolic BPs. An automated stepwise variable-selection procedure was used to develop the final logistic model for predicting in-hospital mortality.
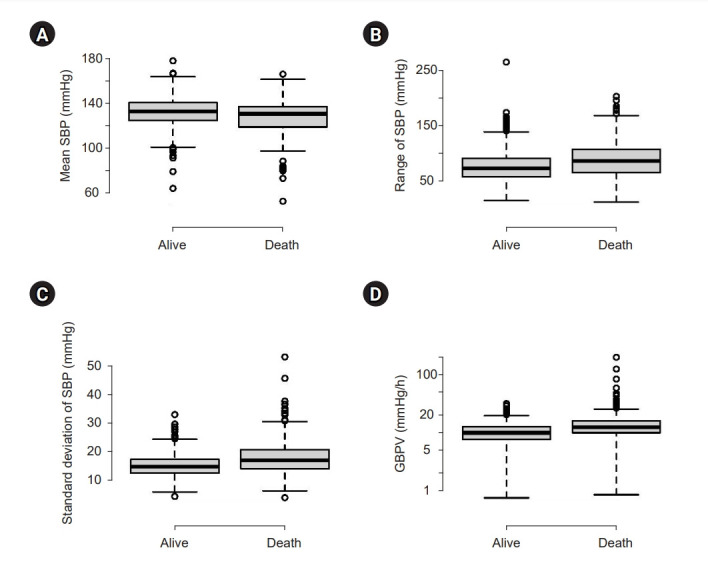
Results: Out of 1,036 patients, 802 (77.4%) survived and were discharged after spontaneous ICH. Factors associated with mortality included age; male sex; ICH in the brainstem, ventricle, or multiple locations; low GCS score (< 9); high NIHSS score (> 20); and diabetes with complications. Mean systolic BP, SD, and GBPV were also linked to mortality. Higher GBPV notably increased the risk of in-hospital death, with an odds ratio of 3.21 (95% confidence interval, 2.10 to 4.97) for every + 10 mmHg/h change in GBPV.
Conclusions: This study underscores the additional impact of GBPV, herein linked to BPV, on mortality following ICH, providing further insights into the management of blood pressure in the early stages of ICH treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


