{"title":"开发用于预测急性胰腺炎患者胰腺门静脉高压的提名图:一项回顾性研究。","authors":"Yingjie Zhang, Qiaoyu Su, Yunling Li, Xianchen Zhan, XiangPing Wang, Linhui Zhang, Hui Luo, Xiaoyu Kang, Yong Lv, Shuhui Liang, Gui Ren, Yanglin Pan","doi":"10.1136/bmjgast-2024-001539","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Pancreatic portal hypertension (PPH) is a rare complication of acute pancreatitis (AP) that can lead to severe gastrointestinal bleeding. The risk factors associated with PPH, as well as the overall prognosis, warrant further investigation. This study aims to develop and validate a nomogram to predict PPH in patients with AP.</p><p><strong>Methods: </strong>Consecutive patients with AP from 2015 to 2023 were retrospectively included in the study. Demographic data, clinical manifestations within the first week of AP onset, and initial contrast-enhanced CT findings were used to develop the predictive model. Univariate and multivariate Cox regression analyses were performed to identify risk factors for PPH. Based on the results of the multivariate analysis, a nomogram was developed. The patients were randomly divided into training and validation sets at a 7:3 ratio. The accuracy and discriminative power of the predictive model were assessed using the area under the curve (AUC) from the receiver operating characteristic curve and the calibration curve.</p><p><strong>Results: </strong>Of the 1473 patients with AP, 107 (7.3%) developed PPH within 6 months (range: 2-22 months) during follow-up. Multivariate regression analysis showed that body mass index (BMI) (HR, 1.10; 95% CI 1.04 to 1.16; p=0.001), moderately severe grade (HR, 9.36; 95% CI 4.58 to 19.13; p<0.001), severe grade (HR, 12.95; 95% CI 6.22 to 26.94; p<0.001), diabetes (HR, 2.26; 95% CI 1.47 to 3.47; p<0.001), acute fluid accumulation (HR, 2.13; 95% CI 1.31 to 3.47; p=0.002), and necrosis (HR, 3.64; 95% CI 2.30 to 5.78; p<0.001) were independent risk factors for PPH. A nomogram for predicting PPH was developed, with the predictive curves showing an AUC of 0.859 at 6 months and 0.846 at 9 months. In the validation set, the AUC at both time points was 0.812.</p><p><strong>Conclusion: </strong>In summary, we identified BMI, moderately severe or severe AP, diabetes, acute fluid accumulation, and necrosis as risk factors for AP-related PPH. Using the largest cohort of patients with AP to date, we developed a highly accurate nomogram with strong discriminative ability for predicting PPH. Future studies with larger sample sizes are necessary to confirm our findings and conduct external validation.</p>","PeriodicalId":9235,"journal":{"name":"BMJ Open Gastroenterology","volume":"11 1","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2024-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11552527/pdf/","citationCount":"0","resultStr":"{\"title\":\"Development of a nomogram for predicting pancreatic portal hypertension in patients with acute pancreatitis: a retrospective study.\",\"authors\":\"Yingjie Zhang, Qiaoyu Su, Yunling Li, Xianchen Zhan, XiangPing Wang, Linhui Zhang, Hui Luo, Xiaoyu Kang, Yong Lv, Shuhui Liang, Gui Ren, Yanglin Pan\",\"doi\":\"10.1136/bmjgast-2024-001539\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Pancreatic portal hypertension (PPH) is a rare complication of acute pancreatitis (AP) that can lead to severe gastrointestinal bleeding. The risk factors associated with PPH, as well as the overall prognosis, warrant further investigation. This study aims to develop and validate a nomogram to predict PPH in patients with AP.</p><p><strong>Methods: </strong>Consecutive patients with AP from 2015 to 2023 were retrospectively included in the study. Demographic data, clinical manifestations within the first week of AP onset, and initial contrast-enhanced CT findings were used to develop the predictive model. Univariate and multivariate Cox regression analyses were performed to identify risk factors for PPH. Based on the results of the multivariate analysis, a nomogram was developed. The patients were randomly divided into training and validation sets at a 7:3 ratio. The accuracy and discriminative power of the predictive model were assessed using the area under the curve (AUC) from the receiver operating characteristic curve and the calibration curve.</p><p><strong>Results: </strong>Of the 1473 patients with AP, 107 (7.3%) developed PPH within 6 months (range: 2-22 months) during follow-up. Multivariate regression analysis showed that body mass index (BMI) (HR, 1.10; 95% CI 1.04 to 1.16; p=0.001), moderately severe grade (HR, 9.36; 95% CI 4.58 to 19.13; p<0.001), severe grade (HR, 12.95; 95% CI 6.22 to 26.94; p<0.001), diabetes (HR, 2.26; 95% CI 1.47 to 3.47; p<0.001), acute fluid accumulation (HR, 2.13; 95% CI 1.31 to 3.47; p=0.002), and necrosis (HR, 3.64; 95% CI 2.30 to 5.78; p<0.001) were independent risk factors for PPH. A nomogram for predicting PPH was developed, with the predictive curves showing an AUC of 0.859 at 6 months and 0.846 at 9 months. In the validation set, the AUC at both time points was 0.812.</p><p><strong>Conclusion: </strong>In summary, we identified BMI, moderately severe or severe AP, diabetes, acute fluid accumulation, and necrosis as risk factors for AP-related PPH. Using the largest cohort of patients with AP to date, we developed a highly accurate nomogram with strong discriminative ability for predicting PPH. Future studies with larger sample sizes are necessary to confirm our findings and conduct external validation.</p>\",\"PeriodicalId\":9235,\"journal\":{\"name\":\"BMJ Open Gastroenterology\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-11-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11552527/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Gastroenterology\",\"FirstCategoryId\":\"88\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjgast-2024-001539\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Gastroenterology","FirstCategoryId":"88","ListUrlMain":"https://doi.org/10.1136/bmjgast-2024-001539","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
简介:胰腺门静脉高压症(PPH)是急性胰腺炎(AP)的一种罕见并发症,可导致严重的消化道出血。与 PPH 相关的风险因素以及总体预后值得进一步研究。本研究旨在开发并验证预测急性胰腺炎患者 PPH 的提名图:本研究回顾性纳入了 2015 年至 2023 年期间的连续 AP 患者。人口统计学数据、AP 发病第一周内的临床表现和初始对比增强 CT 结果被用于开发预测模型。进行了单变量和多变量 Cox 回归分析,以确定 PPH 的风险因素。根据多变量分析的结果,制定了一个提名图。按 7:3 的比例将患者随机分为训练集和验证集。利用接收者操作特征曲线和校准曲线的曲线下面积(AUC)评估了预测模型的准确性和鉴别力:在1473名AP患者中,有107人(7.3%)在随访的6个月内(范围:2-22个月)发生了PPH。多变量回归分析表明,体重指数(BMI)(HR,1.10;95% CI 1.04 至 1.16;P=0.001)、中度重度等级(HR,9.36;95% CI 4.58 至 19.13;P结论:总之,我们发现体重指数、中重度或重度 AP、糖尿病、急性积液和坏死是 AP 相关 PPH 的风险因素。利用迄今为止最大的 AP 患者群,我们开发出了一个高度准确的提名图,对预测 PPH 有很强的鉴别能力。今后有必要进行样本量更大的研究,以证实我们的发现并进行外部验证。
Development of a nomogram for predicting pancreatic portal hypertension in patients with acute pancreatitis: a retrospective study.
Introduction: Pancreatic portal hypertension (PPH) is a rare complication of acute pancreatitis (AP) that can lead to severe gastrointestinal bleeding. The risk factors associated with PPH, as well as the overall prognosis, warrant further investigation. This study aims to develop and validate a nomogram to predict PPH in patients with AP.
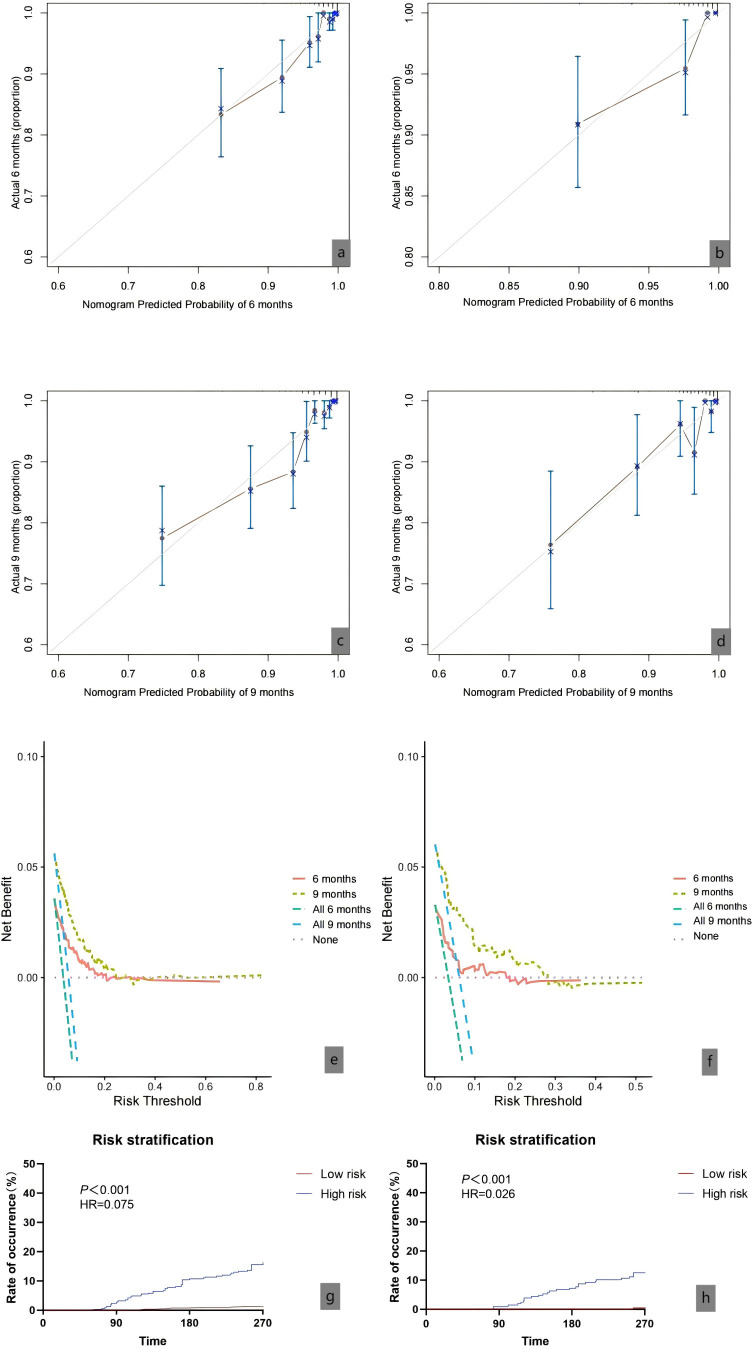
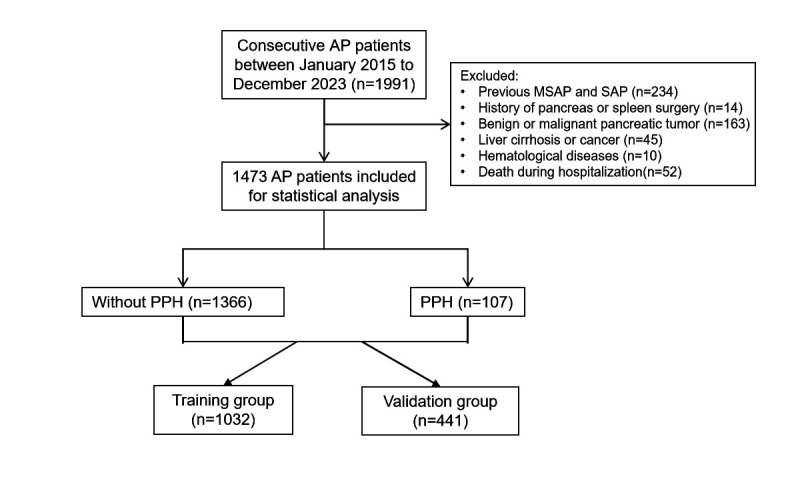
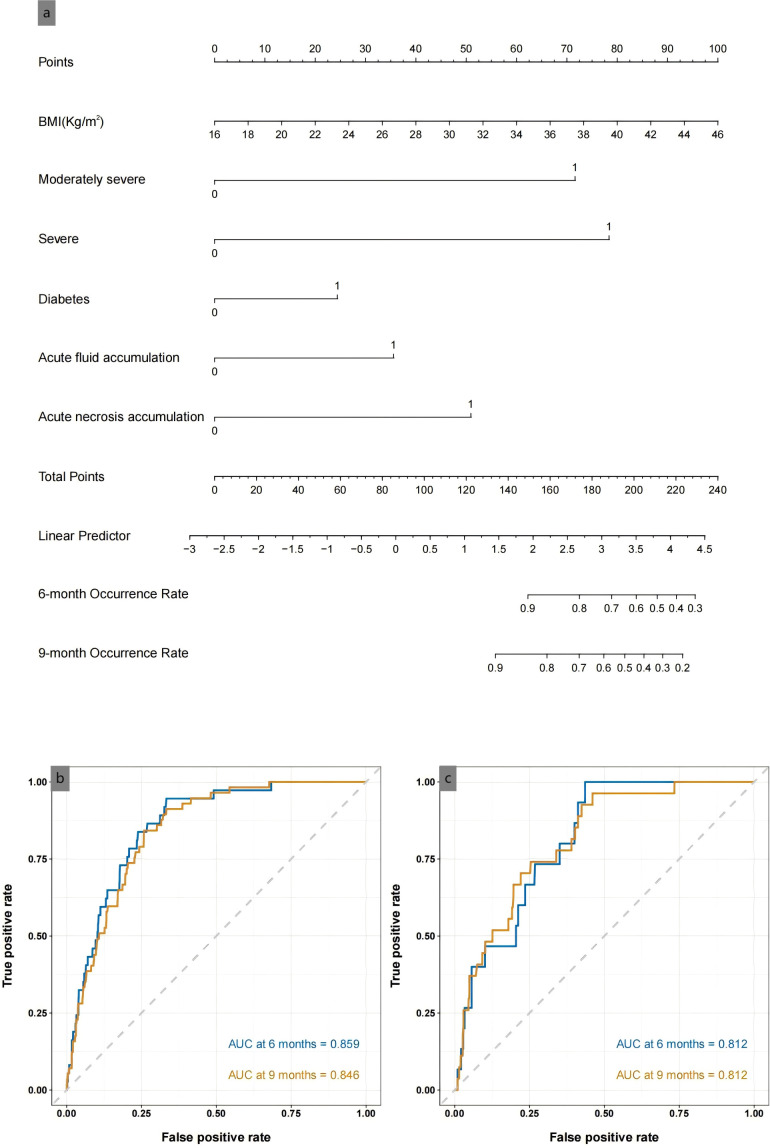
Methods: Consecutive patients with AP from 2015 to 2023 were retrospectively included in the study. Demographic data, clinical manifestations within the first week of AP onset, and initial contrast-enhanced CT findings were used to develop the predictive model. Univariate and multivariate Cox regression analyses were performed to identify risk factors for PPH. Based on the results of the multivariate analysis, a nomogram was developed. The patients were randomly divided into training and validation sets at a 7:3 ratio. The accuracy and discriminative power of the predictive model were assessed using the area under the curve (AUC) from the receiver operating characteristic curve and the calibration curve.
Results: Of the 1473 patients with AP, 107 (7.3%) developed PPH within 6 months (range: 2-22 months) during follow-up. Multivariate regression analysis showed that body mass index (BMI) (HR, 1.10; 95% CI 1.04 to 1.16; p=0.001), moderately severe grade (HR, 9.36; 95% CI 4.58 to 19.13; p<0.001), severe grade (HR, 12.95; 95% CI 6.22 to 26.94; p<0.001), diabetes (HR, 2.26; 95% CI 1.47 to 3.47; p<0.001), acute fluid accumulation (HR, 2.13; 95% CI 1.31 to 3.47; p=0.002), and necrosis (HR, 3.64; 95% CI 2.30 to 5.78; p<0.001) were independent risk factors for PPH. A nomogram for predicting PPH was developed, with the predictive curves showing an AUC of 0.859 at 6 months and 0.846 at 9 months. In the validation set, the AUC at both time points was 0.812.
Conclusion: In summary, we identified BMI, moderately severe or severe AP, diabetes, acute fluid accumulation, and necrosis as risk factors for AP-related PPH. Using the largest cohort of patients with AP to date, we developed a highly accurate nomogram with strong discriminative ability for predicting PPH. Future studies with larger sample sizes are necessary to confirm our findings and conduct external validation.
期刊介绍:
BMJ Open Gastroenterology is an online-only, peer-reviewed, open access gastroenterology journal, dedicated to publishing high-quality medical research from all disciplines and therapeutic areas of gastroenterology. It is the open access companion journal of Gut and is co-owned by the British Society of Gastroenterology. The journal publishes all research study types, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Publishing procedures are built around continuous publication, publishing research online as soon as the article is ready.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


