膀胱癌患者接受输尿管支架术后并发上尿路上皮癌的风险
IF 2.3
3区 医学
Q3 ONCOLOGY
引用次数: 0
摘要
目的关于上尿路(UUT)减压对膀胱癌(BCa)患者 UUT 复发风险的影响的数据很少。本研究旨在评估与经皮肾造瘘术(PCN)相比,双 J 支架置入术(DJS)是否会增加 UUT 复发的风险。材料与方法我们回顾性分析了 12 家三级医疗中心(1990-2020 年)中接受根治性膀胱切除术(RC)的 1550 例 cTa-T3NanyM0 BCa 患者的数据。这些患者均接受过完整的随访,既往无 UUT 癌症史,且术前因肾积水而需要进行 UUT 减压术。肾积水等级根据已建立的评分系统进行定义。UUT 复发通过影像学和尿液细胞学诊断,并在可能的情况下通过选择性细胞学和输尿管镜检查确认。计算倾向评分以确定重叠权重和平衡组别。Kaplan-Meier分析估计了加权前后的UUT无复发生存期(RFS)、癌症特异性生存期(CSS)和总生存期(OS)。结果 在纳入的 524 例患者中,分别有 132 例(25%)和 392 例(75%)患者接受了 DJS 和 PCN 治疗。与接受DJS治疗的患者相比,接受PCN治疗的患者梗阻等级(≥3)(34%对14%)和pT3-4肿瘤(70%对36%)更高。在中位 19 个月的随访期间,两组患者的 2 年 UUT-RFS 无差异(PCN 为 95% vs DJS 为 92%,加权 HR 1.41,95% CI,0.55-3.59)。2年加权CSS(74% vs. 74%)和OS(67% vs. 69%)没有差异。结论这些结果表明,输尿管 DJS 不会增加需要进行 UUT 减压术的 BCa 肾积水患者 UUT 复发的风险。但是,UUT 复发很少见,而且相关性很弱,研究结果容易出现偏差。需要进行随机试验来验证这些结果。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Risk of Metachronous Upper Tract Urothelial Carcinoma After Ureteral Stenting in Patients With Bladder Cancer
Objective
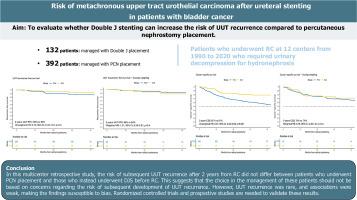
Sparse data exist on the impact of upper urinary tract (UUT) decompression on the risk of UUT recurrence in patients with bladder cancer (BCa). This study aims to evaluate whether Double J stenting (DJS) can increase the risk of UUT recurrence compared to percutaneous nephrostomy (PCN) placement.
Materials and methods
We retrospectively analyzed data from 1550 patients with cTa-T3NanyM0 BCa who underwent radical cystectomy (RC) between at 12 tertiary care centers (1990-2020). Patients with complete follow-up, no prior history of UUT cancer, and who required UUT decompression for preoperative hydronephrosis were selected. Hydronephrosis grade was defined according to established scoring systems. UUT recurrence was diagnosed through imaging, urinary cytology, and confirmed by selective cytology and ureteroscopy when possible. Propensity scores were computed to determine overlap weights and balance groups. Kaplan–Meier analyses estimated UUT recurrence-free survival (RFS), cancer-specific (CSS), and overall survival (OS) before and after weighting. Cox regression analyses before and after weighting were fitted to predict UUT recurrence.
Results
Of 524 included patients, 132 (25%) and 392 (75%) patients were managed with DJS and PCN placement, respectively. Patients who received PCN had higher grade (≥ 3) of obstruction (34% vs. 14%) and pT3-4 tumors (70% vs. 36%) than patients with DJS. During a median follow-up of 19 months, 2-years UUT-RFS did not differ between groups (95% for PCN vs 92% for DJS, weighted HR 1.41, 95% CI, 0.55-3.59). There was no difference in 2-years weighted CSS (74% vs. 74%) and OS (67% vs 69%). Main limitations were the short follow-up and inclusion of patients uniquely undergoing RC.
Conclusions
These results suggest that ureteral DJS does not increase the risk of developing UUT recurrence in BCa patients with hydronephrosis requiring UUT decompression. However, UUT recurrence was rare, and associations were weak, with findings susceptible to bias. Randomized trials are needed to validate these results.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

Clinical genitourinary cancer
医学-泌尿学与肾脏学
CiteScore
5.20
自引率
6.20%
发文量
201
审稿时长
54 days
期刊介绍:
Clinical Genitourinary Cancer is a peer-reviewed journal that publishes original articles describing various aspects of clinical and translational research in genitourinary cancers. Clinical Genitourinary Cancer is devoted to articles on detection, diagnosis, prevention, and treatment of genitourinary cancers. The main emphasis is on recent scientific developments in all areas related to genitourinary malignancies. Specific areas of interest include clinical research and mechanistic approaches; drug sensitivity and resistance; gene and antisense therapy; pathology, markers, and prognostic indicators; chemoprevention strategies; multimodality therapy; and integration of various approaches.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


