腹腔镜方法、早期闭合和术前刺激对直肠切除术后回肠造口闭合效果的影响
IF 1.3
4区 医学
Q3 SURGERY
引用次数: 0
摘要
目的评估在一组主要采用腹腔镜方法进行手术治疗的直肠癌患者中,早期关闭保护性回肠造口并在术前刺激传出肢体的临床效果。方法我们对2017年至2022年期间接受腹腔镜手术并行保护性环形回肠造口术的一系列直肠癌患者进行了一项前瞻性记录的观察性回顾性队列研究。回肠造口关闭计划在术后 3 个月内完成。所有患者都接受了传出肢体刺激。主要结果为发病率和死亡率、住院时间(LOS)和再次入院。结果2017年至2022年间,108名患者接受了直肠癌切除术和保护性回肠造口术。84.3%的患者(n = 91)接受了腹腔镜手术。5名患者(4.6%)接受了永久性回肠造口术。因此,95.4% 的患者(103 人)进行了回肠造口关闭术。中位关闭时间为 74.5 天(57-113 天不等)。63.1%的患者(n = 65)在 90 天内进行了重建手术。77.8%的患者(n = 84)在闭合前接受了传出肢体刺激。总发病率为 26.2%(n = 27)(85.19%,n = 23 例 Clavien-Dindo I 型和 7.41%,n = 2 例 Clavien-Dindo II 型)。发病的主要原因是术后回肠梗阻(10.7%,n = 11)和直肠出血(8.7%,n = 9)。2名患者出现吻合口漏。住院时间中位数为 6 天(5-7 天)。结论 采用腹腔镜方法、早期闭合和刺激传出肢体可能是降低临时回肠造口闭合术发病率和死亡率的有效策略。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Impact of the laparoscopic approach, early closure and preoperative stimulation on outcomes of ileostomy closure after rectal resection
Aim
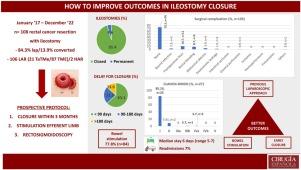
To evaluate the clinical outcome of early closure of a protective ileostomy and preoperative stimulation of the efferent limb in a cohort of patients with rectal cancer treated surgically, primarily using the laparoscopic approach.
Methods
We performed an observational retrospective cohort study in a prospectively recorded series of patients with rectal cancer who underwent laparoscopic surgery with a protective loop ileostomy between 2017 and 2022. Ileostomy closure was programmed for within 3 months after surgery. All patients underwent stimulation of the efferent limb. Primary outcomes were morbidity and mortality, length of stay (LOS), and re-admission.
Results
Between 2017 and 2022, 108 patients underwent resection for rectal cancer and protective ileostomy. The laparoscopic approach was performed in 84.3% of patients (n = 91). Permanent ileostomy was performed in 5 patients (4.6%). Ileostomy closure was thus performed in 95.4% of patients (n = 103). Median time to closure was 74.5 days (range 57–113). In 63.1% (n = 65) of patients, reconstructive surgery was performed within 90 days. Prior to closure, efferent limb stimulation was performed in 77.8% (n = 84) of patients. Global morbidity was 26.2% (n = 27) (85.19%, n = 23 Clavien-Dindo I and 7.41%, n = 2 Clavien-Dindo II). The main causes of morbidity were postoperative ileus (10.7%, n = 11) and rectal bleeding (8.7%, n = 9). Anastomosis leakage occurred in 2 patients. Median hospital stay was 6 days (5–7). Readmission was needed in 6.8% (n = 7) of patients.
Conclusion
A previous laparoscopic approach, early closure and stimulation of the efferent limb could be a useful strategy to reduce the morbidity and mortality of temporary ileostomy closure.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

Cirugia Espanola
SURGERY-
CiteScore
1.20
自引率
21.10%
发文量
173
审稿时长
53 days
期刊介绍:
Cirugía Española, an official body of the Asociación Española de Cirujanos (Spanish Association of Surgeons), will consider original articles, reviews, editorials, special articles, scientific letters, letters to the editor, and medical images for publication; all of these will be submitted to an anonymous external peer review process. There is also the possibility of accepting book reviews of recent publications related to General and Digestive Surgery.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


