Marie Coors, Wiebke Schüttig, Katrin C Reber, Harald Darius, Alfred Holzgreve, Sebastian Karmann, Anica Stürtz, Rebecca Zöller, Saskia Kropp, Petra Riesner, Leonie Sundmacher
{"title":"改善心血管疾病患者护理协调的护士主导过渡护理模式的成本效益和成本效用分析:\"Cardiolotse \"研究的结果。","authors":"Marie Coors, Wiebke Schüttig, Katrin C Reber, Harald Darius, Alfred Holzgreve, Sebastian Karmann, Anica Stürtz, Rebecca Zöller, Saskia Kropp, Petra Riesner, Leonie Sundmacher","doi":"10.1007/s10198-024-01734-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To assess the 12-month cost-effectiveness of the nurse-led transitional care program \"Cardiolotse\" (CL) for patients with cardiovascular diseases compared to usual care (UC).</p><p><strong>Methods: </strong>A cost-effectiveness analysis (CEA) and cost-utility analysis (CUA) were conducted from the perspective of statutory health insurance (SHI), covering a time horizon of 12 months. Analyzed outcomes included the number of rehospitalizations and health-related quality of life (HRQoL). Total costs comprised program costs and the utilization of healthcare resources. Point estimates are presented as incremental cost-effectiveness ratios (ICERs) and incremental cost-utility ratios (ICURs). Sensitivity and subgroup analyses were conducted to illustrate uncertainty and provide insights into the impact mechanisms of the CL program.</p><p><strong>Results: </strong>The study population consisted of 2550 patients, with 1256 allocated to the intervention group and 1294 to the control group. Patients who received support from CLs experienced fewer rehospitalizations and lower inpatient costs from an SHI perspective, compared to the UC group. HRQoL assessments indicated higher utility values for CL patients at the 12-month follow-up. Total program costs amounted to €1454.65 per patient. The CEA and CUA demonstrate that the CL program is dominant compared to UC from the SHI perspective.</p><p><strong>Conclusion: </strong>Our study shows that the CL program not only reduces the number of rehospitalizations and costs but increases HRQoL, resulting in a dominant ICER and ICUR. Further research is necessary to evaluate longer periods of time, different levels of care intensity, and perspectives of different healthcare stakeholders.</p><p><strong>Trial registration: </strong>German Clinical Trial Register DRKS00020424, 2020-06-18, retrospectively registered.</p>","PeriodicalId":51416,"journal":{"name":"European Journal of Health Economics","volume":" ","pages":"697-710"},"PeriodicalIF":3.0000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12204867/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-effectiveness and cost-utility analysis of a nurse-led, transitional care model to improve care coordination for patients with cardiovascular diseases: results from the \\\"Cardiolotse\\\" study.\",\"authors\":\"Marie Coors, Wiebke Schüttig, Katrin C Reber, Harald Darius, Alfred Holzgreve, Sebastian Karmann, Anica Stürtz, Rebecca Zöller, Saskia Kropp, Petra Riesner, Leonie Sundmacher\",\"doi\":\"10.1007/s10198-024-01734-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To assess the 12-month cost-effectiveness of the nurse-led transitional care program \\\"Cardiolotse\\\" (CL) for patients with cardiovascular diseases compared to usual care (UC).</p><p><strong>Methods: </strong>A cost-effectiveness analysis (CEA) and cost-utility analysis (CUA) were conducted from the perspective of statutory health insurance (SHI), covering a time horizon of 12 months. Analyzed outcomes included the number of rehospitalizations and health-related quality of life (HRQoL). Total costs comprised program costs and the utilization of healthcare resources. Point estimates are presented as incremental cost-effectiveness ratios (ICERs) and incremental cost-utility ratios (ICURs). Sensitivity and subgroup analyses were conducted to illustrate uncertainty and provide insights into the impact mechanisms of the CL program.</p><p><strong>Results: </strong>The study population consisted of 2550 patients, with 1256 allocated to the intervention group and 1294 to the control group. Patients who received support from CLs experienced fewer rehospitalizations and lower inpatient costs from an SHI perspective, compared to the UC group. HRQoL assessments indicated higher utility values for CL patients at the 12-month follow-up. Total program costs amounted to €1454.65 per patient. The CEA and CUA demonstrate that the CL program is dominant compared to UC from the SHI perspective.</p><p><strong>Conclusion: </strong>Our study shows that the CL program not only reduces the number of rehospitalizations and costs but increases HRQoL, resulting in a dominant ICER and ICUR. Further research is necessary to evaluate longer periods of time, different levels of care intensity, and perspectives of different healthcare stakeholders.</p><p><strong>Trial registration: </strong>German Clinical Trial Register DRKS00020424, 2020-06-18, retrospectively registered.</p>\",\"PeriodicalId\":51416,\"journal\":{\"name\":\"European Journal of Health Economics\",\"volume\":\" \",\"pages\":\"697-710\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12204867/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Health Economics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10198-024-01734-7\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Health Economics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10198-024-01734-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/6 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
Cost-effectiveness and cost-utility analysis of a nurse-led, transitional care model to improve care coordination for patients with cardiovascular diseases: results from the "Cardiolotse" study.
Objective: To assess the 12-month cost-effectiveness of the nurse-led transitional care program "Cardiolotse" (CL) for patients with cardiovascular diseases compared to usual care (UC).
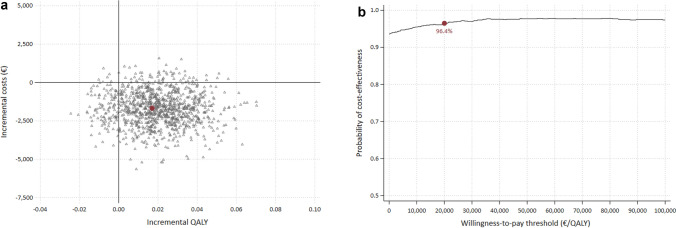
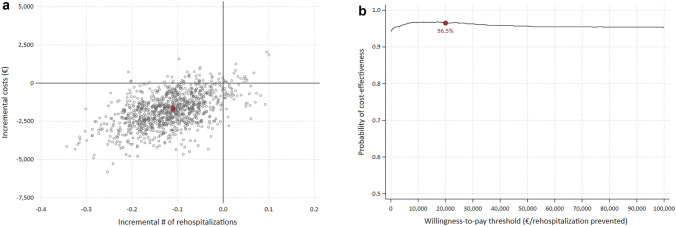
Methods: A cost-effectiveness analysis (CEA) and cost-utility analysis (CUA) were conducted from the perspective of statutory health insurance (SHI), covering a time horizon of 12 months. Analyzed outcomes included the number of rehospitalizations and health-related quality of life (HRQoL). Total costs comprised program costs and the utilization of healthcare resources. Point estimates are presented as incremental cost-effectiveness ratios (ICERs) and incremental cost-utility ratios (ICURs). Sensitivity and subgroup analyses were conducted to illustrate uncertainty and provide insights into the impact mechanisms of the CL program.
Results: The study population consisted of 2550 patients, with 1256 allocated to the intervention group and 1294 to the control group. Patients who received support from CLs experienced fewer rehospitalizations and lower inpatient costs from an SHI perspective, compared to the UC group. HRQoL assessments indicated higher utility values for CL patients at the 12-month follow-up. Total program costs amounted to €1454.65 per patient. The CEA and CUA demonstrate that the CL program is dominant compared to UC from the SHI perspective.
Conclusion: Our study shows that the CL program not only reduces the number of rehospitalizations and costs but increases HRQoL, resulting in a dominant ICER and ICUR. Further research is necessary to evaluate longer periods of time, different levels of care intensity, and perspectives of different healthcare stakeholders.
Trial registration: German Clinical Trial Register DRKS00020424, 2020-06-18, retrospectively registered.
期刊介绍:
The European Journal of Health Economics is a journal of Health Economics and associated disciplines. The growing demand for health economics and the introduction of new guidelines in various European countries were the motivation to generate a highly scientific and at the same time practice oriented journal considering the requirements of various health care systems in Europe. The international scientific board of opinion leaders guarantees high-quality, peer-reviewed publications as well as articles for pragmatic approaches in the field of health economics. We intend to cover all aspects of health economics:
• Basics of health economic approaches and methods
• Pharmacoeconomics
• Health Care Systems
• Pricing and Reimbursement Systems
• Quality-of-Life-Studies The editors reserve the right to reject manuscripts that do not comply with the above-mentioned requirements. The author will be held responsible for false statements or for failure to fulfill the above-mentioned requirements.
Officially cited as: Eur J Health Econ

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


