Xiaoyu Zhang, Tao Xu, Xiaohu An, Jianwei Wang, Qiong Meng, Zifeng Xu
{"title":"在 Narcotrend 和 SPI 监测下,确定瑞芬太尼联合异丙酚用于宫腔镜手术全静脉麻醉的最佳剂量。","authors":"Xiaoyu Zhang, Tao Xu, Xiaohu An, Jianwei Wang, Qiong Meng, Zifeng Xu","doi":"10.1177/20420986241289204","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Outpatient hysteroscopic surgery requires patients to be anaesthetised and recover quickly, and the drugs used must be safe and effective. Remifentanil is typically co-administered with propofol as total intravenous anaesthesia (TIVA) for hysteroscopy because of its favourable pharmacokinetic and pharmacodynamic properties. However, the optimal dose of remifentanil when co-administered with propofol without neuromuscular blocking agents (NMBAs) has not been established.</p><p><strong>Objectives: </strong>In this sequential dose-finding study, the 90% effective dose (ED90) of remifentanil effect-site concentration (Ce) combined with propofol without NMBAs during outpatient hysteroscopy was calculated to minimise the side effects of using higher doses.</p><p><strong>Design: </strong>This sequential dose-finding study was conducted in August 2022.</p><p><strong>Methods: </strong>Forty patients who underwent outpatient hysteroscopy under TIVA were included in the study. With a biased coin up-and-down design, the initial remifentanil Ce was established at 2 ng/mL, and the subsequent remifentanil dosage was determined based on the reaction of the previous patient. The primary outcome was a remifentanil Ce that resulted in successful TIVA by maintaining a Narcotrend index < 60, surgical pleth index (SPI) < 50, and without patient movement throughout hysteroscopy. Secondary outcomes included rates of hypotension-related symptoms and interventions, drug consumption, post-anaesthesia care unit (PACU)-estimated visual analogue scale (VAS) and Ramsay sedation scores, modified Aldrete scores, and other adverse effects of anaesthesia. The ED90 and 95% confidence intervals (CI) were estimated using isotonic regression methods and bootstrapping.</p><p><strong>Results: </strong>For TIVA without NMBAs during outpatient hysteroscopy, the ED90 Ce of remifentanil combined with propofol was determined to be 2.75 ng/mL (95% CI, 2.50-3.00 ng/mL). The incidence of peri-operative adverse effects of anaesthesia was relatively low. All the patients had satisfactory VAS, Ramsay sedation, and modified Aldrete scores in the PACU.</p><p><strong>Conclusion: </strong>Remifentanil at a Ce of 2.75 ng/mL is recommended for TIVA combined with propofol in outpatient hysteroscopic surgery.</p><p><strong>Trial registration: </strong>http://www.chictr.org.cn (ChiCTR2200062284; 31/7/2022).</p>","PeriodicalId":23012,"journal":{"name":"Therapeutic Advances in Drug Safety","volume":"15 ","pages":"20420986241289204"},"PeriodicalIF":3.4000,"publicationDate":"2024-11-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11536375/pdf/","citationCount":"0","resultStr":"{\"title\":\"Determining the optimum dose of remifentanil in combination with propofol for total intravenous anaesthesia in hysteroscopy under Narcotrend and SPI monitoring.\",\"authors\":\"Xiaoyu Zhang, Tao Xu, Xiaohu An, Jianwei Wang, Qiong Meng, Zifeng Xu\",\"doi\":\"10.1177/20420986241289204\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Outpatient hysteroscopic surgery requires patients to be anaesthetised and recover quickly, and the drugs used must be safe and effective. Remifentanil is typically co-administered with propofol as total intravenous anaesthesia (TIVA) for hysteroscopy because of its favourable pharmacokinetic and pharmacodynamic properties. However, the optimal dose of remifentanil when co-administered with propofol without neuromuscular blocking agents (NMBAs) has not been established.</p><p><strong>Objectives: </strong>In this sequential dose-finding study, the 90% effective dose (ED90) of remifentanil effect-site concentration (Ce) combined with propofol without NMBAs during outpatient hysteroscopy was calculated to minimise the side effects of using higher doses.</p><p><strong>Design: </strong>This sequential dose-finding study was conducted in August 2022.</p><p><strong>Methods: </strong>Forty patients who underwent outpatient hysteroscopy under TIVA were included in the study. With a biased coin up-and-down design, the initial remifentanil Ce was established at 2 ng/mL, and the subsequent remifentanil dosage was determined based on the reaction of the previous patient. The primary outcome was a remifentanil Ce that resulted in successful TIVA by maintaining a Narcotrend index < 60, surgical pleth index (SPI) < 50, and without patient movement throughout hysteroscopy. Secondary outcomes included rates of hypotension-related symptoms and interventions, drug consumption, post-anaesthesia care unit (PACU)-estimated visual analogue scale (VAS) and Ramsay sedation scores, modified Aldrete scores, and other adverse effects of anaesthesia. The ED90 and 95% confidence intervals (CI) were estimated using isotonic regression methods and bootstrapping.</p><p><strong>Results: </strong>For TIVA without NMBAs during outpatient hysteroscopy, the ED90 Ce of remifentanil combined with propofol was determined to be 2.75 ng/mL (95% CI, 2.50-3.00 ng/mL). The incidence of peri-operative adverse effects of anaesthesia was relatively low. All the patients had satisfactory VAS, Ramsay sedation, and modified Aldrete scores in the PACU.</p><p><strong>Conclusion: </strong>Remifentanil at a Ce of 2.75 ng/mL is recommended for TIVA combined with propofol in outpatient hysteroscopic surgery.</p><p><strong>Trial registration: </strong>http://www.chictr.org.cn (ChiCTR2200062284; 31/7/2022).</p>\",\"PeriodicalId\":23012,\"journal\":{\"name\":\"Therapeutic Advances in Drug Safety\",\"volume\":\"15 \",\"pages\":\"20420986241289204\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-11-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11536375/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Drug Safety\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/20420986241289204\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20420986241289204","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Determining the optimum dose of remifentanil in combination with propofol for total intravenous anaesthesia in hysteroscopy under Narcotrend and SPI monitoring.
Background: Outpatient hysteroscopic surgery requires patients to be anaesthetised and recover quickly, and the drugs used must be safe and effective. Remifentanil is typically co-administered with propofol as total intravenous anaesthesia (TIVA) for hysteroscopy because of its favourable pharmacokinetic and pharmacodynamic properties. However, the optimal dose of remifentanil when co-administered with propofol without neuromuscular blocking agents (NMBAs) has not been established.
Objectives: In this sequential dose-finding study, the 90% effective dose (ED90) of remifentanil effect-site concentration (Ce) combined with propofol without NMBAs during outpatient hysteroscopy was calculated to minimise the side effects of using higher doses.
Design: This sequential dose-finding study was conducted in August 2022.
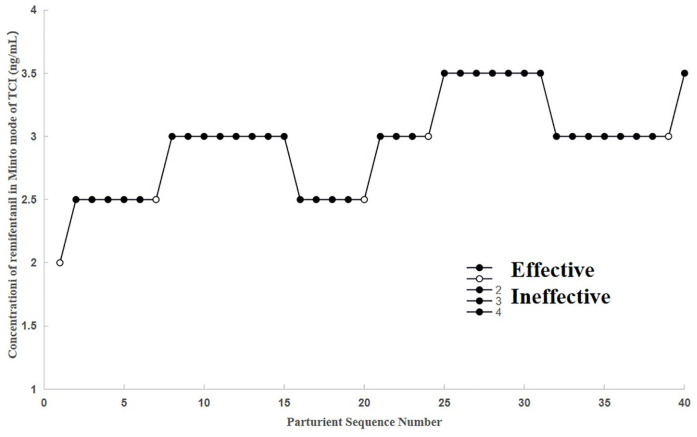
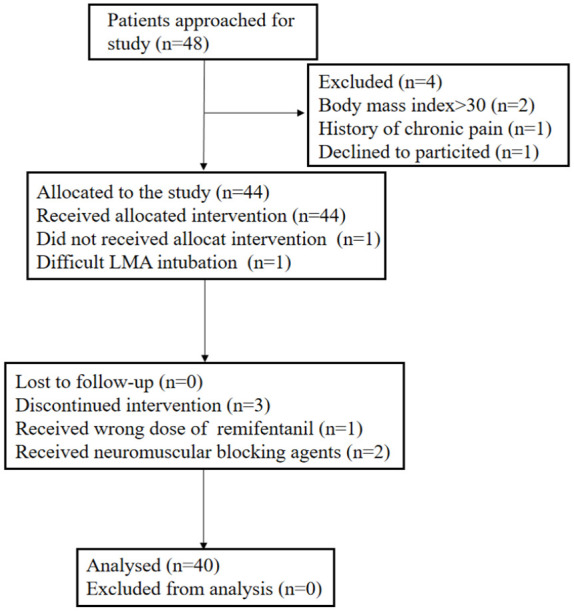
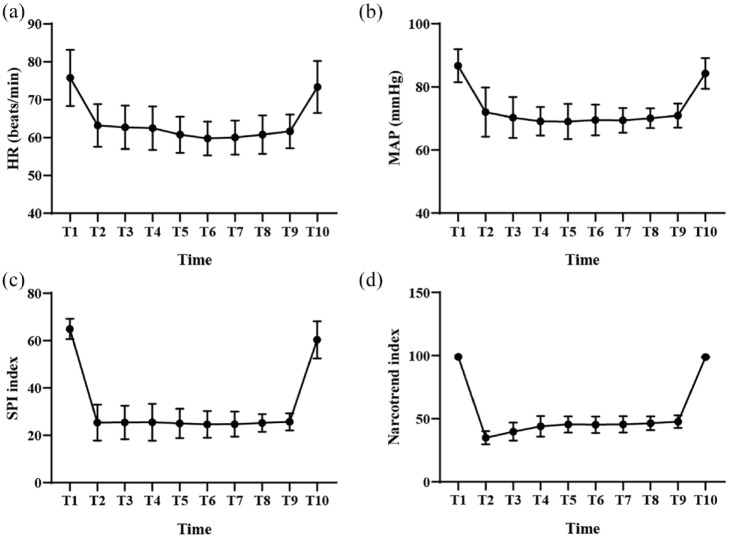
Methods: Forty patients who underwent outpatient hysteroscopy under TIVA were included in the study. With a biased coin up-and-down design, the initial remifentanil Ce was established at 2 ng/mL, and the subsequent remifentanil dosage was determined based on the reaction of the previous patient. The primary outcome was a remifentanil Ce that resulted in successful TIVA by maintaining a Narcotrend index < 60, surgical pleth index (SPI) < 50, and without patient movement throughout hysteroscopy. Secondary outcomes included rates of hypotension-related symptoms and interventions, drug consumption, post-anaesthesia care unit (PACU)-estimated visual analogue scale (VAS) and Ramsay sedation scores, modified Aldrete scores, and other adverse effects of anaesthesia. The ED90 and 95% confidence intervals (CI) were estimated using isotonic regression methods and bootstrapping.
Results: For TIVA without NMBAs during outpatient hysteroscopy, the ED90 Ce of remifentanil combined with propofol was determined to be 2.75 ng/mL (95% CI, 2.50-3.00 ng/mL). The incidence of peri-operative adverse effects of anaesthesia was relatively low. All the patients had satisfactory VAS, Ramsay sedation, and modified Aldrete scores in the PACU.
Conclusion: Remifentanil at a Ce of 2.75 ng/mL is recommended for TIVA combined with propofol in outpatient hysteroscopic surgery.
期刊介绍:
Therapeutic Advances in Drug Safety delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies pertaining to the safe use of drugs in patients.
The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in drug safety, providing a forum in print and online for publishing the highest quality articles in this area. The editors welcome articles of current interest on research across all areas of drug safety, including therapeutic drug monitoring, pharmacoepidemiology, adverse drug reactions, drug interactions, pharmacokinetics, pharmacovigilance, medication/prescribing errors, risk management, ethics and regulation.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


