Héloïse Bannelier, Thomas Kapfer, Mélanie Roussel, Yonathan Freund, Karine Alame, Pierre Catoire, Amélie Vromant
{"title":"肺栓塞高临床可能性患者的 D-二聚体检测失败率:三项欧洲研究的辅助分析。","authors":"Héloïse Bannelier, Thomas Kapfer, Mélanie Roussel, Yonathan Freund, Karine Alame, Pierre Catoire, Amélie Vromant","doi":"10.1111/acem.15032","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In patients with a high clinical probability of pulmonary embolism (PE), the high prevalence can lower the D-dimer negative predictive value and increase the risk of diagnostic failure. It is therefore recommended that these high-risk patients should undergo chest imaging without D-dimer testing although no evidence supports this recommendation.</p><p><strong>Objective: </strong>The objective was to evaluate the safety of ruling out PE based on D-dimer testing among patients with a high clinical probability of PE.</p><p><strong>Methods: </strong>This was a post hoc analysis of three European studies (PROPER, MODIGLIANI, and TRYSPEED). Patients were included if they presented a high clinical probability of PE (according to either the Wells or the revised Geneva score) and underwent D-dimer testing. The D-dimer-based strategy ruled out PE if the D-dimer level was below the age-adjusted threshold (i.e., <500 ng/mL in patients aged less than 50 and age × 10 ng/mL in patients older than 50). The primary endpoint was a thromboembolic event in patients with negative D-dimer either at index visit or at 3-month follow-up. A Bayesian approach estimated the probability that the failure rate of the D-dimer-based strategy was below 2% given observed data.</p><p><strong>Results: </strong>Among the 12,300 patients included in the PROPER, MODIGLIANI, and TRYSPEED studies, 651 patients (median age 68 years, 60% female) had D-dimer testing and a high clinical probability of PE and were included in the study. PE prevalence was 31.3%. Seventy patients had D-dimer levels under the age-adjusted threshold, and none of them had a PE after follow-up (failure rate 0.0% [95% CI 0.0%-6.5%]). Bayesian analysis reported a credible interval of 0.0%-4.1%, with a 76.2% posterior probability of a failure rate below 2%.</p><p><strong>Conclusions: </strong>In this study, ruling out PE in high-risk patients based on D-dimer below the age-adjusted threshold was safe, with no missed PE. However, the large CI of the primary endpoint precludes a definitive conclusion.</p>","PeriodicalId":7105,"journal":{"name":"Academic Emergency Medicine","volume":" ","pages":"116-122"},"PeriodicalIF":3.2000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11816009/pdf/","citationCount":"0","resultStr":"{\"title\":\"Failure rate of D-dimer testing in patients with high clinical probability of pulmonary embolism: Ancillary analysis of three European studies.\",\"authors\":\"Héloïse Bannelier, Thomas Kapfer, Mélanie Roussel, Yonathan Freund, Karine Alame, Pierre Catoire, Amélie Vromant\",\"doi\":\"10.1111/acem.15032\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In patients with a high clinical probability of pulmonary embolism (PE), the high prevalence can lower the D-dimer negative predictive value and increase the risk of diagnostic failure. It is therefore recommended that these high-risk patients should undergo chest imaging without D-dimer testing although no evidence supports this recommendation.</p><p><strong>Objective: </strong>The objective was to evaluate the safety of ruling out PE based on D-dimer testing among patients with a high clinical probability of PE.</p><p><strong>Methods: </strong>This was a post hoc analysis of three European studies (PROPER, MODIGLIANI, and TRYSPEED). Patients were included if they presented a high clinical probability of PE (according to either the Wells or the revised Geneva score) and underwent D-dimer testing. The D-dimer-based strategy ruled out PE if the D-dimer level was below the age-adjusted threshold (i.e., <500 ng/mL in patients aged less than 50 and age × 10 ng/mL in patients older than 50). The primary endpoint was a thromboembolic event in patients with negative D-dimer either at index visit or at 3-month follow-up. A Bayesian approach estimated the probability that the failure rate of the D-dimer-based strategy was below 2% given observed data.</p><p><strong>Results: </strong>Among the 12,300 patients included in the PROPER, MODIGLIANI, and TRYSPEED studies, 651 patients (median age 68 years, 60% female) had D-dimer testing and a high clinical probability of PE and were included in the study. PE prevalence was 31.3%. Seventy patients had D-dimer levels under the age-adjusted threshold, and none of them had a PE after follow-up (failure rate 0.0% [95% CI 0.0%-6.5%]). Bayesian analysis reported a credible interval of 0.0%-4.1%, with a 76.2% posterior probability of a failure rate below 2%.</p><p><strong>Conclusions: </strong>In this study, ruling out PE in high-risk patients based on D-dimer below the age-adjusted threshold was safe, with no missed PE. However, the large CI of the primary endpoint precludes a definitive conclusion.</p>\",\"PeriodicalId\":7105,\"journal\":{\"name\":\"Academic Emergency Medicine\",\"volume\":\" \",\"pages\":\"116-122\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2025-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11816009/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Academic Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/acem.15032\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Academic Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/acem.15032","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景:在临床上肺栓塞(PE)可能性较高的患者中,高患病率会降低 D-二聚体的阴性预测值,增加诊断失败的风险。因此,尽管没有证据支持这一建议,但仍建议这些高危患者在不进行 D-二聚体检测的情况下进行胸部成像:目的:评估临床上很可能患有 PE 的患者根据 D-二聚体检测排除 PE 的安全性:这是对三项欧洲研究(PROPER、MODIGLIANI 和 TRYSPEED)的事后分析。临床上极有可能发生 PE 的患者(根据韦尔斯评分或修订后的日内瓦评分)均被纳入研究范围,并接受了 D-二聚体检测。如果 D-二聚体水平低于年龄调整后的阈值(即结果),则基于 D-二聚体的策略将 PE 排除在外:在 PROPER、MODIGLIANI 和 TRYSPEED 研究的 12,300 名患者中,有 651 名患者(中位年龄为 68 岁,60% 为女性)接受了 D-二聚体检测,临床上发生 PE 的可能性很高,因此被纳入研究。PE 患病率为 31.3%。70名患者的D-二聚体水平低于年龄调整后的阈值,随访后无一人发生PE(失败率为0.0% [95% CI 0.0%-6.5%])。贝叶斯分析报告的可信区间为0.0%-4.1%,失败率低于2%的后验概率为76.2%:在这项研究中,根据低于年龄调整阈值的 D-二聚体排除高危患者的 PE 是安全的,没有漏诊 PE。然而,由于主要终点的CI值较大,因此无法得出明确的结论。
Failure rate of D-dimer testing in patients with high clinical probability of pulmonary embolism: Ancillary analysis of three European studies.
Background: In patients with a high clinical probability of pulmonary embolism (PE), the high prevalence can lower the D-dimer negative predictive value and increase the risk of diagnostic failure. It is therefore recommended that these high-risk patients should undergo chest imaging without D-dimer testing although no evidence supports this recommendation.
Objective: The objective was to evaluate the safety of ruling out PE based on D-dimer testing among patients with a high clinical probability of PE.
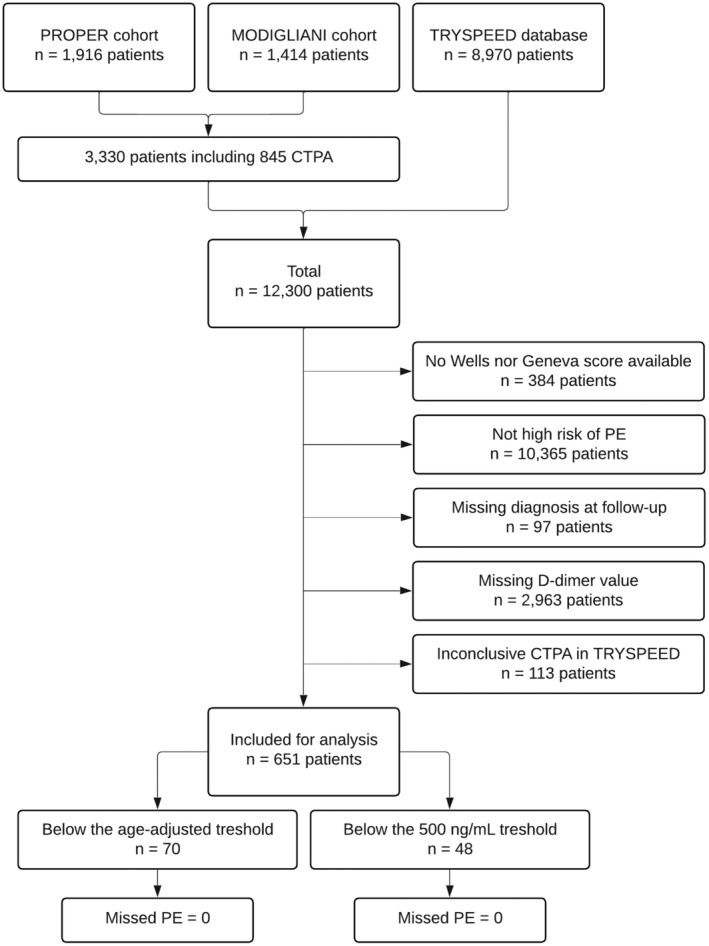
Methods: This was a post hoc analysis of three European studies (PROPER, MODIGLIANI, and TRYSPEED). Patients were included if they presented a high clinical probability of PE (according to either the Wells or the revised Geneva score) and underwent D-dimer testing. The D-dimer-based strategy ruled out PE if the D-dimer level was below the age-adjusted threshold (i.e., <500 ng/mL in patients aged less than 50 and age × 10 ng/mL in patients older than 50). The primary endpoint was a thromboembolic event in patients with negative D-dimer either at index visit or at 3-month follow-up. A Bayesian approach estimated the probability that the failure rate of the D-dimer-based strategy was below 2% given observed data.
Results: Among the 12,300 patients included in the PROPER, MODIGLIANI, and TRYSPEED studies, 651 patients (median age 68 years, 60% female) had D-dimer testing and a high clinical probability of PE and were included in the study. PE prevalence was 31.3%. Seventy patients had D-dimer levels under the age-adjusted threshold, and none of them had a PE after follow-up (failure rate 0.0% [95% CI 0.0%-6.5%]). Bayesian analysis reported a credible interval of 0.0%-4.1%, with a 76.2% posterior probability of a failure rate below 2%.
Conclusions: In this study, ruling out PE in high-risk patients based on D-dimer below the age-adjusted threshold was safe, with no missed PE. However, the large CI of the primary endpoint precludes a definitive conclusion.
期刊介绍:
Academic Emergency Medicine (AEM) is the official monthly publication of the Society for Academic Emergency Medicine (SAEM) and publishes information relevant to the practice, educational advancements, and investigation of emergency medicine. It is the second-largest peer-reviewed scientific journal in the specialty of emergency medicine.
The goal of AEM is to advance the science, education, and clinical practice of emergency medicine, to serve as a voice for the academic emergency medicine community, and to promote SAEM''s goals and objectives. Members and non-members worldwide depend on this journal for translational medicine relevant to emergency medicine, as well as for clinical news, case studies and more.
Each issue contains information relevant to the research, educational advancements, and practice in emergency medicine. Subject matter is diverse, including preclinical studies, clinical topics, health policy, and educational methods. The research of SAEM members contributes significantly to the scientific content and development of the journal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


