Areeba Abid MD, Michelle P. Lin MD, Elizabeth Cox MD, Timothy J. Batchelor MD
{"title":"一名突发性单侧视力丧失的妇女","authors":"Areeba Abid MD, Michelle P. Lin MD, Elizabeth Cox MD, Timothy J. Batchelor MD","doi":"10.1002/emp2.13337","DOIUrl":null,"url":null,"abstract":"<p>A 60-year-old female with a history of breast cancer in remission presented to the emergency department with 1 day of acute onset left eye visual changes, which she described as “shadows” and “tunnel-like.” She reported mild pain and “stinging” with extraocular movements of the left eye. Physical exam demonstrated relative afferent pupillary defect in the left eye, with visual field defects in the infranasal and supratemporal regions. The patient had normal intraocular pressure (IOP) and 20/20 corrected central vision. Ocular point-of-care ultrasound of the left eye was performed, demonstrating “spot sign” (Figure 1, Video 1). The presumptive diagnosis was corroborated by a comprehensive ocular examination by ophthalmology. She was ultimately discharged to outpatient follow up on dual-antiplatelet therapy.</p><p><i>Central retinal artery occlusion</i> (CRAO) typically presents with painless loss of vision,<span><sup>1</sup></span> resulting from sudden blockage of the central retinal artery. This is an ocular emergency and a stroke equivalent, with retinal hypoperfusion causing rapidly progressive retinal damage and vision loss.<span><sup>2</sup></span></p><p>“Spot sign” is a hyperechoic focus sometimes seen posterior to the globe within the optic nerve sheath, indicative of a calcified embolus from atherosclerotic plaques. Transbulbar ultrasound is valuable for the initial diagnosis and workup of CRAO because it helps to elucidate whether occlusion is secondary to thrombus or calcified embolus, with positive spot sign associated with decreased effectiveness of thrombolysis. The absence of spot sign may help to identify patients more likely to benefit from thrombolytic treatment.<span><sup>3</sup></span></p><p>We wish to confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome. We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us. We confirm that we have given due consideration to the protection of intellectual property associated with this work and that there are no impediments to publication, including the timing of publication, with respect to intellectual property. In so doing, we confirm that we have followed the regulations of our institutions concerning intellectual property and patient confidentiality. We understand that the corresponding author is the sole contact for the editorial process (including editorial manager and direct communications with the office). She is responsible for communicating with the other authors about progress, submissions of revisions, and final approval of proofs.</p><p>We confirm that we have provided a current, correct email address which is accessible by the Corresponding Author and which has been configured to accept email at <span>[email protected]</span>.</p>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 6","pages":""},"PeriodicalIF":1.6000,"publicationDate":"2024-10-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13337","citationCount":"0","resultStr":"{\"title\":\"A woman with sudden unilateral vision loss\",\"authors\":\"Areeba Abid MD, Michelle P. Lin MD, Elizabeth Cox MD, Timothy J. Batchelor MD\",\"doi\":\"10.1002/emp2.13337\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 60-year-old female with a history of breast cancer in remission presented to the emergency department with 1 day of acute onset left eye visual changes, which she described as “shadows” and “tunnel-like.” She reported mild pain and “stinging” with extraocular movements of the left eye. Physical exam demonstrated relative afferent pupillary defect in the left eye, with visual field defects in the infranasal and supratemporal regions. The patient had normal intraocular pressure (IOP) and 20/20 corrected central vision. Ocular point-of-care ultrasound of the left eye was performed, demonstrating “spot sign” (Figure 1, Video 1). The presumptive diagnosis was corroborated by a comprehensive ocular examination by ophthalmology. She was ultimately discharged to outpatient follow up on dual-antiplatelet therapy.</p><p><i>Central retinal artery occlusion</i> (CRAO) typically presents with painless loss of vision,<span><sup>1</sup></span> resulting from sudden blockage of the central retinal artery. This is an ocular emergency and a stroke equivalent, with retinal hypoperfusion causing rapidly progressive retinal damage and vision loss.<span><sup>2</sup></span></p><p>“Spot sign” is a hyperechoic focus sometimes seen posterior to the globe within the optic nerve sheath, indicative of a calcified embolus from atherosclerotic plaques. Transbulbar ultrasound is valuable for the initial diagnosis and workup of CRAO because it helps to elucidate whether occlusion is secondary to thrombus or calcified embolus, with positive spot sign associated with decreased effectiveness of thrombolysis. The absence of spot sign may help to identify patients more likely to benefit from thrombolytic treatment.<span><sup>3</sup></span></p><p>We wish to confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome. We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us. We confirm that we have given due consideration to the protection of intellectual property associated with this work and that there are no impediments to publication, including the timing of publication, with respect to intellectual property. In so doing, we confirm that we have followed the regulations of our institutions concerning intellectual property and patient confidentiality. We understand that the corresponding author is the sole contact for the editorial process (including editorial manager and direct communications with the office). She is responsible for communicating with the other authors about progress, submissions of revisions, and final approval of proofs.</p><p>We confirm that we have provided a current, correct email address which is accessible by the Corresponding Author and which has been configured to accept email at <span>[email protected]</span>.</p>\",\"PeriodicalId\":73967,\"journal\":{\"name\":\"Journal of the American College of Emergency Physicians open\",\"volume\":\"5 6\",\"pages\":\"\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2024-10-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13337\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American College of Emergency Physicians open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13337\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13337","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
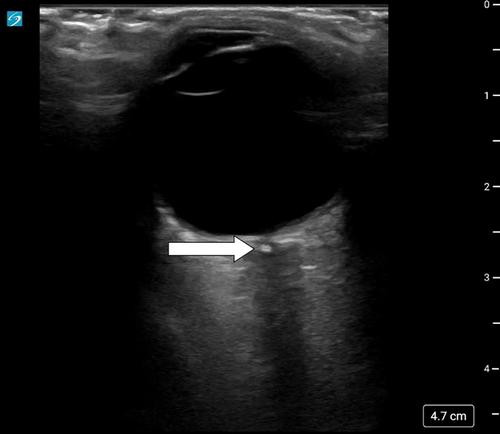
A 60-year-old female with a history of breast cancer in remission presented to the emergency department with 1 day of acute onset left eye visual changes, which she described as “shadows” and “tunnel-like.” She reported mild pain and “stinging” with extraocular movements of the left eye. Physical exam demonstrated relative afferent pupillary defect in the left eye, with visual field defects in the infranasal and supratemporal regions. The patient had normal intraocular pressure (IOP) and 20/20 corrected central vision. Ocular point-of-care ultrasound of the left eye was performed, demonstrating “spot sign” (Figure 1, Video 1). The presumptive diagnosis was corroborated by a comprehensive ocular examination by ophthalmology. She was ultimately discharged to outpatient follow up on dual-antiplatelet therapy.
Central retinal artery occlusion (CRAO) typically presents with painless loss of vision,1 resulting from sudden blockage of the central retinal artery. This is an ocular emergency and a stroke equivalent, with retinal hypoperfusion causing rapidly progressive retinal damage and vision loss.2
“Spot sign” is a hyperechoic focus sometimes seen posterior to the globe within the optic nerve sheath, indicative of a calcified embolus from atherosclerotic plaques. Transbulbar ultrasound is valuable for the initial diagnosis and workup of CRAO because it helps to elucidate whether occlusion is secondary to thrombus or calcified embolus, with positive spot sign associated with decreased effectiveness of thrombolysis. The absence of spot sign may help to identify patients more likely to benefit from thrombolytic treatment.3
We wish to confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome. We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us. We confirm that we have given due consideration to the protection of intellectual property associated with this work and that there are no impediments to publication, including the timing of publication, with respect to intellectual property. In so doing, we confirm that we have followed the regulations of our institutions concerning intellectual property and patient confidentiality. We understand that the corresponding author is the sole contact for the editorial process (including editorial manager and direct communications with the office). She is responsible for communicating with the other authors about progress, submissions of revisions, and final approval of proofs.
We confirm that we have provided a current, correct email address which is accessible by the Corresponding Author and which has been configured to accept email at [email protected].

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


