Ivancarmine Gambardella, Berhane Worku, Christopher Lau, Robert Tranbaugh, Sandhya Balaram, Leonard Girardi
{"title":"糖尿病可预测主动脉弓置换术后的严重呼吸衰竭","authors":"Ivancarmine Gambardella, Berhane Worku, Christopher Lau, Robert Tranbaugh, Sandhya Balaram, Leonard Girardi","doi":"10.1155/2024/3776969","DOIUrl":null,"url":null,"abstract":"<div>\n <p><b>Objective:</b> The lung is a target organ of diabetes mellitus (DM) via glycation of pulmonary elastin and collagen. In addition, hyperglycemia facilitates hypercapnic respiratory failure, which is instead mitigated by low-carbohydrate high-lipid (LC-HL) nutrition. We sought to determine the association between diabetes and severe respiratory failure (SRF, i.e., need of reintubation\\tracheostomy) after open aortic arch replacement (AAR).</p>\n <p><b>Methods:</b> Machine learning algorithms were evaluated for precision and recall (F2 score) and for clinical applicability to predict SRF. Conditional regression evaluated independent predictors of SRF after 1:2 propensity-score matching.</p>\n <p><b>Results:</b> Information on diabetic status was available in 1275 patients undergoing AAR (1997–2023). Although support vector machine presented the highest F2 score (<i>F</i>2 = 0.337), conditional inference trees provided the most clinically applicable algorithm: diabetes was the best predictor of SRF, which occurred in 20/150 diabetics (13.3%) vs. 40/1125 nondiabetics (3.6%) (<i>p</i> < 0.01). In diabetics, left ventricular ejection fraction (LVEF) was the next best predictor of SRF, which occurred in 8/20 diabetics with LVEF ≤ 30% (40%) vs. 12/130 diabetics with LVEF >30% (9.2%) (<i>p</i> = 0.02). In nondiabetics, chronic obstructive pulmonary disease (COPD) was the next best predictor of respiratory failure, which occurred in 14/177 nondiabetics with COPD (7.9%) vs. 26/948 nondiabetics without COPD (2.7%) (<i>p</i> = 0.01). In the matched sample, diabetes was independently able to predict SRF (OR 2.20, 95% CI 1.10 | 4.42).</p>\n <p><b>Conclusions:</b> DM was the best predictor of SRF after AAR. Strict glycemic control and LC-HL nutrition should be evaluated as measures to reduce postoperative SRF in diabetic patients.</p>\n </div>","PeriodicalId":15367,"journal":{"name":"Journal of Cardiac Surgery","volume":"2024 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2024-10-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/3776969","citationCount":"0","resultStr":"{\"title\":\"Diabetes Mellitus Predicts Severe Respiratory Failure After Aortic Arch Replacement\",\"authors\":\"Ivancarmine Gambardella, Berhane Worku, Christopher Lau, Robert Tranbaugh, Sandhya Balaram, Leonard Girardi\",\"doi\":\"10.1155/2024/3776969\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n <p><b>Objective:</b> The lung is a target organ of diabetes mellitus (DM) via glycation of pulmonary elastin and collagen. In addition, hyperglycemia facilitates hypercapnic respiratory failure, which is instead mitigated by low-carbohydrate high-lipid (LC-HL) nutrition. We sought to determine the association between diabetes and severe respiratory failure (SRF, i.e., need of reintubation\\\\tracheostomy) after open aortic arch replacement (AAR).</p>\\n <p><b>Methods:</b> Machine learning algorithms were evaluated for precision and recall (F2 score) and for clinical applicability to predict SRF. Conditional regression evaluated independent predictors of SRF after 1:2 propensity-score matching.</p>\\n <p><b>Results:</b> Information on diabetic status was available in 1275 patients undergoing AAR (1997–2023). Although support vector machine presented the highest F2 score (<i>F</i>2 = 0.337), conditional inference trees provided the most clinically applicable algorithm: diabetes was the best predictor of SRF, which occurred in 20/150 diabetics (13.3%) vs. 40/1125 nondiabetics (3.6%) (<i>p</i> < 0.01). In diabetics, left ventricular ejection fraction (LVEF) was the next best predictor of SRF, which occurred in 8/20 diabetics with LVEF ≤ 30% (40%) vs. 12/130 diabetics with LVEF >30% (9.2%) (<i>p</i> = 0.02). In nondiabetics, chronic obstructive pulmonary disease (COPD) was the next best predictor of respiratory failure, which occurred in 14/177 nondiabetics with COPD (7.9%) vs. 26/948 nondiabetics without COPD (2.7%) (<i>p</i> = 0.01). In the matched sample, diabetes was independently able to predict SRF (OR 2.20, 95% CI 1.10 | 4.42).</p>\\n <p><b>Conclusions:</b> DM was the best predictor of SRF after AAR. Strict glycemic control and LC-HL nutrition should be evaluated as measures to reduce postoperative SRF in diabetic patients.</p>\\n </div>\",\"PeriodicalId\":15367,\"journal\":{\"name\":\"Journal of Cardiac Surgery\",\"volume\":\"2024 1\",\"pages\":\"\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-10-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/3776969\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiac Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1155/2024/3776969\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiac Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/3776969","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Diabetes Mellitus Predicts Severe Respiratory Failure After Aortic Arch Replacement
Objective: The lung is a target organ of diabetes mellitus (DM) via glycation of pulmonary elastin and collagen. In addition, hyperglycemia facilitates hypercapnic respiratory failure, which is instead mitigated by low-carbohydrate high-lipid (LC-HL) nutrition. We sought to determine the association between diabetes and severe respiratory failure (SRF, i.e., need of reintubation\tracheostomy) after open aortic arch replacement (AAR).
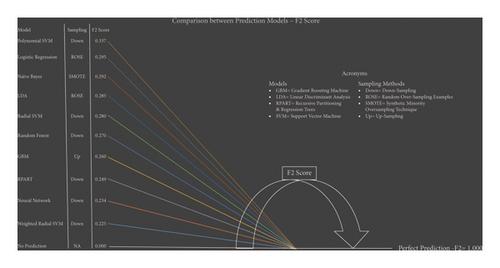
Methods: Machine learning algorithms were evaluated for precision and recall (F2 score) and for clinical applicability to predict SRF. Conditional regression evaluated independent predictors of SRF after 1:2 propensity-score matching.
Results: Information on diabetic status was available in 1275 patients undergoing AAR (1997–2023). Although support vector machine presented the highest F2 score (F2 = 0.337), conditional inference trees provided the most clinically applicable algorithm: diabetes was the best predictor of SRF, which occurred in 20/150 diabetics (13.3%) vs. 40/1125 nondiabetics (3.6%) (p < 0.01). In diabetics, left ventricular ejection fraction (LVEF) was the next best predictor of SRF, which occurred in 8/20 diabetics with LVEF ≤ 30% (40%) vs. 12/130 diabetics with LVEF >30% (9.2%) (p = 0.02). In nondiabetics, chronic obstructive pulmonary disease (COPD) was the next best predictor of respiratory failure, which occurred in 14/177 nondiabetics with COPD (7.9%) vs. 26/948 nondiabetics without COPD (2.7%) (p = 0.01). In the matched sample, diabetes was independently able to predict SRF (OR 2.20, 95% CI 1.10 | 4.42).
Conclusions: DM was the best predictor of SRF after AAR. Strict glycemic control and LC-HL nutrition should be evaluated as measures to reduce postoperative SRF in diabetic patients.
期刊介绍:
Journal of Cardiac Surgery (JCS) is a peer-reviewed journal devoted to contemporary surgical treatment of cardiac disease. Renown for its detailed "how to" methods, JCS''s well-illustrated, concise technical articles, critical reviews and commentaries are highly valued by dedicated readers worldwide.
With Editor-in-Chief Harold Lazar, MD and an internationally prominent editorial board, JCS continues its 20-year history as an important professional resource. Editorial coverage includes biologic support, mechanical cardiac assist and/or replacement and surgical techniques, and features current material on topics such as OPCAB surgery, stented and stentless valves, endovascular stent placement, atrial fibrillation, transplantation, percutaneous valve repair/replacement, left ventricular restoration surgery, immunobiology, and bridges to transplant and recovery.
In addition, special sections (Images in Cardiac Surgery, Cardiac Regeneration) and historical reviews stimulate reader interest. The journal also routinely publishes proceedings of important international symposia in a timely manner.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


