Gustavo Casas Aparicio, Rosario Fernández Plata, Anjarath Higuera Iglesias, David Martínez Briseño, Rolando Claure-Del Granado, Manuel Castillejos Lopez, Joel Vázquez Pérez, Noé Alvarado Vásquez, Rafael Velázquez Cruz, Graciela Hernández Silva, Victor Ruiz, Ángel Camarena, Citlaltepetl Salinas Lara, Martha Tena Suck, Iñaki Montes de Oca Ambriz, Oswaldo Ortiz Toledo, Vianey Arvizu Serrano, Yared Almazan Chaparro, Edgar Flores-Soto, Luz María Torres-Espíndola, Arnoldo Aquino-Gálvez, Victor Hugo Ahumada Topete
{"title":"严重 COVID-19 患者血尿素氮/血清肌酐比值(PI-BUN/Cr)持续升高的临床意义。","authors":"Gustavo Casas Aparicio, Rosario Fernández Plata, Anjarath Higuera Iglesias, David Martínez Briseño, Rolando Claure-Del Granado, Manuel Castillejos Lopez, Joel Vázquez Pérez, Noé Alvarado Vásquez, Rafael Velázquez Cruz, Graciela Hernández Silva, Victor Ruiz, Ángel Camarena, Citlaltepetl Salinas Lara, Martha Tena Suck, Iñaki Montes de Oca Ambriz, Oswaldo Ortiz Toledo, Vianey Arvizu Serrano, Yared Almazan Chaparro, Edgar Flores-Soto, Luz María Torres-Espíndola, Arnoldo Aquino-Gálvez, Victor Hugo Ahumada Topete","doi":"10.1186/s41479-024-00140-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with COVID-19 may experience a persistent increase in the blood urea nitrogen over creatinine ratio (PI-BUN/Cr). Its elevation could reflect multiple underlying pathophysiological processes beyond prerenal injury but also warrants nuanced interpretation due to its complex interplay with various factors, underscoring the importance of investigating its effects on mortality and acute kidney injury in this population.</p><p><strong>Methods: </strong>We analized a retrospective and longitudinal cohort of patients admitted to a single center in Mexico City for patients with severe COVID-19. Between March 5, 2020 and August 25, 2021, we included patients with confirmed positive diagnosis for SARS-CoV-2, age > 18 years, disease severity was defined by clinical data of respiratory distress syndrome and a ratio of partial oxygen pressure to inspired oxygen fraction < 300 mmHg on admission. We excluded patients with End Stage Kidney Disease. Data was obtained from electronic medical records. PI-BUN/Cr was defined as an increase in the BUN/Cr ratio > 30 in more than 60% of measurements in the hospital. The outcomes included: risk factors to mortality and AKI in-hospital.</p><p><strong>Results: </strong>The cohort included 3,007 patients with a median age of 54.6 ± 14.5 years. 35% of patients died; 44.6% developed PI-BUN/Cr ratio and 71.4% AKI. Mortality was associated with older age > 60 years [Hazard ratio (HR)] = 1.45, 95% CI: 1.28-1.65; p < 0.001); male (HR 1.25, 95% CI 1.09-1.44; p = 0.002) and AKI (HR 3.29, 95% CI 2.42-4.46; p < 0.001); PI-BUN/CR & Non-AKI (HR = 2.82, 95% CI: 1.61-4.93; p < 0.001); Non PI-BUN/CR & AKI (HR = 5.47, 95% CI: 3.54-8.44; p < 0.001); and PI-BUN/CR & AKI (HR = 4.26, 95% CI: 2.75-6.62, p < 0.001). Only hiperuricemia was a risk factor for AKI (HR = 1.71, 95% CI: 1.30-2.25, p < 0.001).</p><p><strong>Conclusions: </strong>While PI-BUN/Cr alone may not directly associate with mortality, its capacity to sub-phenotype patients according to their AKI status holds significant promise in offering valuable insights into patient prognosis and outcomes. Understanding the nuanced relationship between PI-BUN/Cr and AKI enhances our comprehension of renal function dynamics. It equips healthcare providers with a refined tool for risk stratification and personalized patient management strategies.</p>","PeriodicalId":45120,"journal":{"name":"Pneumonia","volume":"16 1","pages":"20"},"PeriodicalIF":6.2000,"publicationDate":"2024-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11515407/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical implications of persistently increased blood urea nitrogen/serum creatinine ratio (PI-BUN/Cr) in severe COVID-19 patients.\",\"authors\":\"Gustavo Casas Aparicio, Rosario Fernández Plata, Anjarath Higuera Iglesias, David Martínez Briseño, Rolando Claure-Del Granado, Manuel Castillejos Lopez, Joel Vázquez Pérez, Noé Alvarado Vásquez, Rafael Velázquez Cruz, Graciela Hernández Silva, Victor Ruiz, Ángel Camarena, Citlaltepetl Salinas Lara, Martha Tena Suck, Iñaki Montes de Oca Ambriz, Oswaldo Ortiz Toledo, Vianey Arvizu Serrano, Yared Almazan Chaparro, Edgar Flores-Soto, Luz María Torres-Espíndola, Arnoldo Aquino-Gálvez, Victor Hugo Ahumada Topete\",\"doi\":\"10.1186/s41479-024-00140-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients with COVID-19 may experience a persistent increase in the blood urea nitrogen over creatinine ratio (PI-BUN/Cr). Its elevation could reflect multiple underlying pathophysiological processes beyond prerenal injury but also warrants nuanced interpretation due to its complex interplay with various factors, underscoring the importance of investigating its effects on mortality and acute kidney injury in this population.</p><p><strong>Methods: </strong>We analized a retrospective and longitudinal cohort of patients admitted to a single center in Mexico City for patients with severe COVID-19. Between March 5, 2020 and August 25, 2021, we included patients with confirmed positive diagnosis for SARS-CoV-2, age > 18 years, disease severity was defined by clinical data of respiratory distress syndrome and a ratio of partial oxygen pressure to inspired oxygen fraction < 300 mmHg on admission. We excluded patients with End Stage Kidney Disease. Data was obtained from electronic medical records. PI-BUN/Cr was defined as an increase in the BUN/Cr ratio > 30 in more than 60% of measurements in the hospital. The outcomes included: risk factors to mortality and AKI in-hospital.</p><p><strong>Results: </strong>The cohort included 3,007 patients with a median age of 54.6 ± 14.5 years. 35% of patients died; 44.6% developed PI-BUN/Cr ratio and 71.4% AKI. Mortality was associated with older age > 60 years [Hazard ratio (HR)] = 1.45, 95% CI: 1.28-1.65; p < 0.001); male (HR 1.25, 95% CI 1.09-1.44; p = 0.002) and AKI (HR 3.29, 95% CI 2.42-4.46; p < 0.001); PI-BUN/CR & Non-AKI (HR = 2.82, 95% CI: 1.61-4.93; p < 0.001); Non PI-BUN/CR & AKI (HR = 5.47, 95% CI: 3.54-8.44; p < 0.001); and PI-BUN/CR & AKI (HR = 4.26, 95% CI: 2.75-6.62, p < 0.001). Only hiperuricemia was a risk factor for AKI (HR = 1.71, 95% CI: 1.30-2.25, p < 0.001).</p><p><strong>Conclusions: </strong>While PI-BUN/Cr alone may not directly associate with mortality, its capacity to sub-phenotype patients according to their AKI status holds significant promise in offering valuable insights into patient prognosis and outcomes. Understanding the nuanced relationship between PI-BUN/Cr and AKI enhances our comprehension of renal function dynamics. It equips healthcare providers with a refined tool for risk stratification and personalized patient management strategies.</p>\",\"PeriodicalId\":45120,\"journal\":{\"name\":\"Pneumonia\",\"volume\":\"16 1\",\"pages\":\"20\"},\"PeriodicalIF\":6.2000,\"publicationDate\":\"2024-10-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11515407/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pneumonia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41479-024-00140-0\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pneumonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41479-024-00140-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Clinical implications of persistently increased blood urea nitrogen/serum creatinine ratio (PI-BUN/Cr) in severe COVID-19 patients.
Background: Patients with COVID-19 may experience a persistent increase in the blood urea nitrogen over creatinine ratio (PI-BUN/Cr). Its elevation could reflect multiple underlying pathophysiological processes beyond prerenal injury but also warrants nuanced interpretation due to its complex interplay with various factors, underscoring the importance of investigating its effects on mortality and acute kidney injury in this population.
Methods: We analized a retrospective and longitudinal cohort of patients admitted to a single center in Mexico City for patients with severe COVID-19. Between March 5, 2020 and August 25, 2021, we included patients with confirmed positive diagnosis for SARS-CoV-2, age > 18 years, disease severity was defined by clinical data of respiratory distress syndrome and a ratio of partial oxygen pressure to inspired oxygen fraction < 300 mmHg on admission. We excluded patients with End Stage Kidney Disease. Data was obtained from electronic medical records. PI-BUN/Cr was defined as an increase in the BUN/Cr ratio > 30 in more than 60% of measurements in the hospital. The outcomes included: risk factors to mortality and AKI in-hospital.
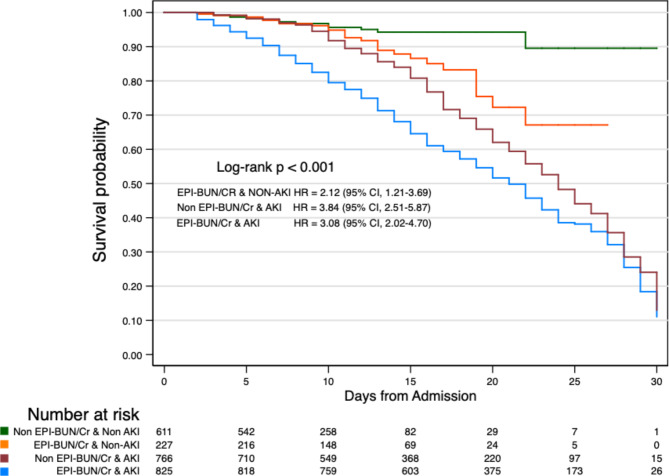
Results: The cohort included 3,007 patients with a median age of 54.6 ± 14.5 years. 35% of patients died; 44.6% developed PI-BUN/Cr ratio and 71.4% AKI. Mortality was associated with older age > 60 years [Hazard ratio (HR)] = 1.45, 95% CI: 1.28-1.65; p < 0.001); male (HR 1.25, 95% CI 1.09-1.44; p = 0.002) and AKI (HR 3.29, 95% CI 2.42-4.46; p < 0.001); PI-BUN/CR & Non-AKI (HR = 2.82, 95% CI: 1.61-4.93; p < 0.001); Non PI-BUN/CR & AKI (HR = 5.47, 95% CI: 3.54-8.44; p < 0.001); and PI-BUN/CR & AKI (HR = 4.26, 95% CI: 2.75-6.62, p < 0.001). Only hiperuricemia was a risk factor for AKI (HR = 1.71, 95% CI: 1.30-2.25, p < 0.001).
Conclusions: While PI-BUN/Cr alone may not directly associate with mortality, its capacity to sub-phenotype patients according to their AKI status holds significant promise in offering valuable insights into patient prognosis and outcomes. Understanding the nuanced relationship between PI-BUN/Cr and AKI enhances our comprehension of renal function dynamics. It equips healthcare providers with a refined tool for risk stratification and personalized patient management strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



