Marc Sicova, Ryan McGinn, Sophia Emerson, Paula Perez, Roberto Gonzalez, Yanhong Li, Olusegum Famure, Ian Randall, Daniel Santa Mina, Michael Santema, Duminda N. Wijeysundera, Wilton Van Klei, S. Joseph Kim, Stuart A. McCluskey
{"title":"术中低血压与肾移植后移植物功能延迟的关系:单中心回顾性队列研究","authors":"Marc Sicova, Ryan McGinn, Sophia Emerson, Paula Perez, Roberto Gonzalez, Yanhong Li, Olusegum Famure, Ian Randall, Daniel Santa Mina, Michael Santema, Duminda N. Wijeysundera, Wilton Van Klei, S. Joseph Kim, Stuart A. McCluskey","doi":"10.1111/ctr.70000","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Intraoperative hypotension is associated with acute kidney injury after surgery. However, the definition (duration and magnitude) of hypotension during kidney transplantation (KT) surgery on early graft function remains unclear.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We conducted a retrospective cohort study of KT recipients from December 1, 2009, to December 31, 2019. Exposure to intraoperative hypotension was characterized as the duration (minutes) of mean arterial pressure (MAP) <55, <65, <75, and <85 mmHg. Our co-primary outcomes were DGF-creatinine reduction ratio (DGF-CRR, <30% creatinine reduction, postoperative days 1 and 2), and DGF-dialysis (DGF-D, required dialysis within the week of KT for deceased donor recipients). Logistic regression models were fitted to assess this relationship between MAP and DGF.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We included 1602 KT (939 deceased donors, 663 living donors) and 23 were excluded. DGF-CRR occurred in 33% of patients. DGF-CRR was associated with MAP < 65 (>5 min: OR 1.77, 95% confidence interval [CI]: 1.39–2.30; 6–10 min: OR 1.67, 95% CI: 0.97–2.86; 11–20 min: OR 2.18, 95% CI: 1.31–3.63) in unadjusted and <55 mmHg (5 min: OR 1.85, 95% CI: 1.47–2.32; 5–10 min: OR 2.41, 95% CI: 1.65–3.53; 11–20 min: OR 2.36, 95% CI: 1.60, 3.48) in adjusted models. There was also a signal for increased risk of DGF-CRR at MAP < 75 (>5 min: OR 1.69, 95% CI: 1.02–2.80). DGF-D (incidence 35%) in deceased donor KT was not associated with hypotension.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>We found an association between intraoperative hypotension and DGF-CRR at a threshold MAP of 55 mmHg, with a consistent signal toward increased risk at both 65 and 75 mmHg, as indicated by unadjusted models.</p>\n </section>\n </div>","PeriodicalId":10467,"journal":{"name":"Clinical Transplantation","volume":"38 10","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-10-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.70000","citationCount":"0","resultStr":"{\"title\":\"Association of Intraoperative Hypotension With Delayed Graft Function Following Kidney Transplant: A Single Centre Retrospective Cohort Study\",\"authors\":\"Marc Sicova, Ryan McGinn, Sophia Emerson, Paula Perez, Roberto Gonzalez, Yanhong Li, Olusegum Famure, Ian Randall, Daniel Santa Mina, Michael Santema, Duminda N. Wijeysundera, Wilton Van Klei, S. Joseph Kim, Stuart A. McCluskey\",\"doi\":\"10.1111/ctr.70000\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Intraoperative hypotension is associated with acute kidney injury after surgery. However, the definition (duration and magnitude) of hypotension during kidney transplantation (KT) surgery on early graft function remains unclear.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We conducted a retrospective cohort study of KT recipients from December 1, 2009, to December 31, 2019. Exposure to intraoperative hypotension was characterized as the duration (minutes) of mean arterial pressure (MAP) <55, <65, <75, and <85 mmHg. Our co-primary outcomes were DGF-creatinine reduction ratio (DGF-CRR, <30% creatinine reduction, postoperative days 1 and 2), and DGF-dialysis (DGF-D, required dialysis within the week of KT for deceased donor recipients). Logistic regression models were fitted to assess this relationship between MAP and DGF.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>We included 1602 KT (939 deceased donors, 663 living donors) and 23 were excluded. DGF-CRR occurred in 33% of patients. DGF-CRR was associated with MAP < 65 (>5 min: OR 1.77, 95% confidence interval [CI]: 1.39–2.30; 6–10 min: OR 1.67, 95% CI: 0.97–2.86; 11–20 min: OR 2.18, 95% CI: 1.31–3.63) in unadjusted and <55 mmHg (5 min: OR 1.85, 95% CI: 1.47–2.32; 5–10 min: OR 2.41, 95% CI: 1.65–3.53; 11–20 min: OR 2.36, 95% CI: 1.60, 3.48) in adjusted models. There was also a signal for increased risk of DGF-CRR at MAP < 75 (>5 min: OR 1.69, 95% CI: 1.02–2.80). DGF-D (incidence 35%) in deceased donor KT was not associated with hypotension.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>We found an association between intraoperative hypotension and DGF-CRR at a threshold MAP of 55 mmHg, with a consistent signal toward increased risk at both 65 and 75 mmHg, as indicated by unadjusted models.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10467,\"journal\":{\"name\":\"Clinical Transplantation\",\"volume\":\"38 10\",\"pages\":\"\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-10-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.70000\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Transplantation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ctr.70000\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Transplantation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ctr.70000","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
Association of Intraoperative Hypotension With Delayed Graft Function Following Kidney Transplant: A Single Centre Retrospective Cohort Study
Background
Intraoperative hypotension is associated with acute kidney injury after surgery. However, the definition (duration and magnitude) of hypotension during kidney transplantation (KT) surgery on early graft function remains unclear.
Methods
We conducted a retrospective cohort study of KT recipients from December 1, 2009, to December 31, 2019. Exposure to intraoperative hypotension was characterized as the duration (minutes) of mean arterial pressure (MAP) <55, <65, <75, and <85 mmHg. Our co-primary outcomes were DGF-creatinine reduction ratio (DGF-CRR, <30% creatinine reduction, postoperative days 1 and 2), and DGF-dialysis (DGF-D, required dialysis within the week of KT for deceased donor recipients). Logistic regression models were fitted to assess this relationship between MAP and DGF.
Results
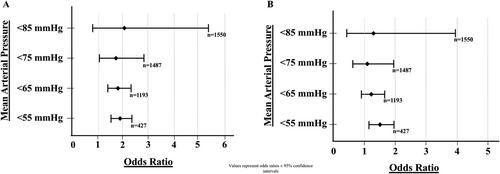
We included 1602 KT (939 deceased donors, 663 living donors) and 23 were excluded. DGF-CRR occurred in 33% of patients. DGF-CRR was associated with MAP < 65 (>5 min: OR 1.77, 95% confidence interval [CI]: 1.39–2.30; 6–10 min: OR 1.67, 95% CI: 0.97–2.86; 11–20 min: OR 2.18, 95% CI: 1.31–3.63) in unadjusted and <55 mmHg (5 min: OR 1.85, 95% CI: 1.47–2.32; 5–10 min: OR 2.41, 95% CI: 1.65–3.53; 11–20 min: OR 2.36, 95% CI: 1.60, 3.48) in adjusted models. There was also a signal for increased risk of DGF-CRR at MAP < 75 (>5 min: OR 1.69, 95% CI: 1.02–2.80). DGF-D (incidence 35%) in deceased donor KT was not associated with hypotension.
Conclusions
We found an association between intraoperative hypotension and DGF-CRR at a threshold MAP of 55 mmHg, with a consistent signal toward increased risk at both 65 and 75 mmHg, as indicated by unadjusted models.
期刊介绍:
Clinical Transplantation: The Journal of Clinical and Translational Research aims to serve as a channel of rapid communication for all those involved in the care of patients who require, or have had, organ or tissue transplants, including: kidney, intestine, liver, pancreas, islets, heart, heart valves, lung, bone marrow, cornea, skin, bone, and cartilage, viable or stored.
Published monthly, Clinical Transplantation’s scope is focused on the complete spectrum of present transplant therapies, as well as also those that are experimental or may become possible in future. Topics include:
Immunology and immunosuppression;
Patient preparation;
Social, ethical, and psychological issues;
Complications, short- and long-term results;
Artificial organs;
Donation and preservation of organ and tissue;
Translational studies;
Advances in tissue typing;
Updates on transplant pathology;.
Clinical and translational studies are particularly welcome, as well as focused reviews. Full-length papers and short communications are invited. Clinical reviews are encouraged, as well as seminal papers in basic science which might lead to immediate clinical application. Prominence is regularly given to the results of cooperative surveys conducted by the organ and tissue transplant registries.
Clinical Transplantation: The Journal of Clinical and Translational Research is essential reading for clinicians and researchers in the diverse field of transplantation: surgeons; clinical immunologists; cryobiologists; hematologists; gastroenterologists; hepatologists; pulmonologists; nephrologists; cardiologists; and endocrinologists. It will also be of interest to sociologists, psychologists, research workers, and to all health professionals whose combined efforts will improve the prognosis of transplant recipients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


