Diego Rivas-Otero, Tomás González-Vidal, Pedro Pujante Alarcón, Elías Delgado Álvarez, Edelmiro Menéndez Torre
{"title":"继发于创伤性脑损伤的垂体前叶功能减退症引起的肌水肿昏迷。","authors":"Diego Rivas-Otero, Tomás González-Vidal, Pedro Pujante Alarcón, Elías Delgado Álvarez, Edelmiro Menéndez Torre","doi":"10.1155/2024/3588840","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background/Objective:</b> Myxedema coma typically presents with decreased level of consciousness and hypothermia, often due to thyroid pathology. In central causes, normal thyroid-stimulating hormone (TSH) levels may delay diagnosis. The purpose of this report is to describe a patient with a history of head trauma who presented with myxedema coma as a manifestation of panhypopituitarism. <b>Case Report:</b> The admitted patient was a 52-year-old man who presented with mental and physical slowness, drowsiness, and weakness. He also had hypotension, hypoglycemia, and low oxygen saturation. Initial evaluation revealed severe pericardial and bilateral pleural effusions, plasma TSH of 2.42 mU/L (normal range 0.25-5.00 mU/L), and plasma adrenocorticotropic hormone (ACTH) of 7.1 pg/mL (normal range 5.2-40.3 pg/mL). Later, his condition deteriorated with anasarca and coma. Signs of improvement were noted after intravenous corticosteroid administration. A subsequent blood test was conducted, which showed a free thyroxine (FT4) level of 0.14 ng/dL (normal range 0.93-1.70 ng/dL). A cranial magnetic resonance scan revealed posttraumatic lesions. The patient's family later admitted head injuries at home. Treatment with intravenous levothyroxine was initiated, resulting in improvement and subsequent discharge in perfect alertness. <b>Conclusion:</b> Hypopituitarism should be suspected in patients with head trauma and symptoms of hormone deficiency. Advanced clinical forms, such as myxedema coma, may also occur. Pituitary hormone levels might be in the normal range, so target gland hormones should be assessed to reach a diagnosis. In the case of suspected central hypothyroidism, requesting only TSH levels may result in a missed diagnosis. For this reason, both TSH and FT4 levels should be measured when central hypothyroidism is suspected.</p>","PeriodicalId":9621,"journal":{"name":"Case Reports in Endocrinology","volume":"2024 ","pages":"3588840"},"PeriodicalIF":0.9000,"publicationDate":"2024-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11498969/pdf/","citationCount":"0","resultStr":"{\"title\":\"Myxedema Coma as a Presentation of Panhypopituitarism Secondary to Traumatic Brain Injury.\",\"authors\":\"Diego Rivas-Otero, Tomás González-Vidal, Pedro Pujante Alarcón, Elías Delgado Álvarez, Edelmiro Menéndez Torre\",\"doi\":\"10.1155/2024/3588840\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background/Objective:</b> Myxedema coma typically presents with decreased level of consciousness and hypothermia, often due to thyroid pathology. In central causes, normal thyroid-stimulating hormone (TSH) levels may delay diagnosis. The purpose of this report is to describe a patient with a history of head trauma who presented with myxedema coma as a manifestation of panhypopituitarism. <b>Case Report:</b> The admitted patient was a 52-year-old man who presented with mental and physical slowness, drowsiness, and weakness. He also had hypotension, hypoglycemia, and low oxygen saturation. Initial evaluation revealed severe pericardial and bilateral pleural effusions, plasma TSH of 2.42 mU/L (normal range 0.25-5.00 mU/L), and plasma adrenocorticotropic hormone (ACTH) of 7.1 pg/mL (normal range 5.2-40.3 pg/mL). Later, his condition deteriorated with anasarca and coma. Signs of improvement were noted after intravenous corticosteroid administration. A subsequent blood test was conducted, which showed a free thyroxine (FT4) level of 0.14 ng/dL (normal range 0.93-1.70 ng/dL). A cranial magnetic resonance scan revealed posttraumatic lesions. The patient's family later admitted head injuries at home. Treatment with intravenous levothyroxine was initiated, resulting in improvement and subsequent discharge in perfect alertness. <b>Conclusion:</b> Hypopituitarism should be suspected in patients with head trauma and symptoms of hormone deficiency. Advanced clinical forms, such as myxedema coma, may also occur. Pituitary hormone levels might be in the normal range, so target gland hormones should be assessed to reach a diagnosis. In the case of suspected central hypothyroidism, requesting only TSH levels may result in a missed diagnosis. For this reason, both TSH and FT4 levels should be measured when central hypothyroidism is suspected.</p>\",\"PeriodicalId\":9621,\"journal\":{\"name\":\"Case Reports in Endocrinology\",\"volume\":\"2024 \",\"pages\":\"3588840\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-10-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11498969/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2024/3588840\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/3588840","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Myxedema Coma as a Presentation of Panhypopituitarism Secondary to Traumatic Brain Injury.
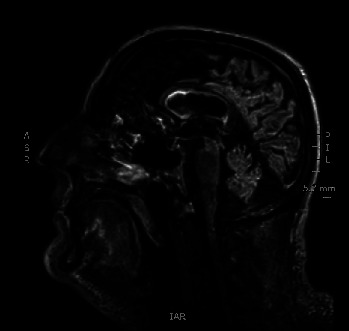
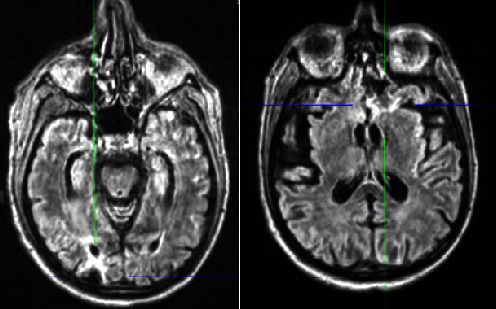
Background/Objective: Myxedema coma typically presents with decreased level of consciousness and hypothermia, often due to thyroid pathology. In central causes, normal thyroid-stimulating hormone (TSH) levels may delay diagnosis. The purpose of this report is to describe a patient with a history of head trauma who presented with myxedema coma as a manifestation of panhypopituitarism. Case Report: The admitted patient was a 52-year-old man who presented with mental and physical slowness, drowsiness, and weakness. He also had hypotension, hypoglycemia, and low oxygen saturation. Initial evaluation revealed severe pericardial and bilateral pleural effusions, plasma TSH of 2.42 mU/L (normal range 0.25-5.00 mU/L), and plasma adrenocorticotropic hormone (ACTH) of 7.1 pg/mL (normal range 5.2-40.3 pg/mL). Later, his condition deteriorated with anasarca and coma. Signs of improvement were noted after intravenous corticosteroid administration. A subsequent blood test was conducted, which showed a free thyroxine (FT4) level of 0.14 ng/dL (normal range 0.93-1.70 ng/dL). A cranial magnetic resonance scan revealed posttraumatic lesions. The patient's family later admitted head injuries at home. Treatment with intravenous levothyroxine was initiated, resulting in improvement and subsequent discharge in perfect alertness. Conclusion: Hypopituitarism should be suspected in patients with head trauma and symptoms of hormone deficiency. Advanced clinical forms, such as myxedema coma, may also occur. Pituitary hormone levels might be in the normal range, so target gland hormones should be assessed to reach a diagnosis. In the case of suspected central hypothyroidism, requesting only TSH levels may result in a missed diagnosis. For this reason, both TSH and FT4 levels should be measured when central hypothyroidism is suspected.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


