Mohamed Sobhy, Adel Eletriby, Hany Ragy, Hossam Kandil, Mohamed Ayman Saleh, Nabil Farag, Ramez Guindy, Ahmed Bendary, Ahmed Mohamed Elmahmoudy Nayel, Ahmed Shawky, Ayman Khairy, Ayman Mortada, Bassem Zarif, Haitham Badran, Hazem Khorshid, Kareem Mahmoud, Karim Said, Khaled Leon, Mahmoud Abdelsabour, Mazen Tawfik, Mohamed Aboel-Kassem F Abdelmegid, Mohamed Koriem, Mohamed Loutfi, Moheb Wadie, Mohamed Elnoamany, Mohamed Sadaka, Mohamed Seleem, Mohamed Zahran, Osama A Amin, Sameh Elkaffas, Sherif Ayad, Wael El Kilany, Walid Ammar, Waleed Elawady, Walid Elhammady, Yasser Abdelhady
{"title":"用于心血管疾病一级和二级预防的 ACE 抑制剂和血管紧张素受体阻滞剂:2024 年埃及心脏病学专家共识与 CVREP 基金会合作提出的建议。","authors":"Mohamed Sobhy, Adel Eletriby, Hany Ragy, Hossam Kandil, Mohamed Ayman Saleh, Nabil Farag, Ramez Guindy, Ahmed Bendary, Ahmed Mohamed Elmahmoudy Nayel, Ahmed Shawky, Ayman Khairy, Ayman Mortada, Bassem Zarif, Haitham Badran, Hazem Khorshid, Kareem Mahmoud, Karim Said, Khaled Leon, Mahmoud Abdelsabour, Mazen Tawfik, Mohamed Aboel-Kassem F Abdelmegid, Mohamed Koriem, Mohamed Loutfi, Moheb Wadie, Mohamed Elnoamany, Mohamed Sadaka, Mohamed Seleem, Mohamed Zahran, Osama A Amin, Sameh Elkaffas, Sherif Ayad, Wael El Kilany, Walid Ammar, Waleed Elawady, Walid Elhammady, Yasser Abdelhady","doi":"10.1007/s40119-024-00381-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The renin-angiotensin-aldosterone system (RAAS) plays a pivotal role in regulating blood pressure (BP), with dysregulation of RAAS resulting in hypertension and potentially heart failure (HF), myocardial infarction (MI), cardio-renal syndrome, and stroke. RAAS inhibitors, such as angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs), have advantages beyond BP control. However, differences between these two drug classes need to be considered when choosing a therapy for preventing cardiovascular events.</p><p><strong>Methods: </strong>A panel of 36 Egyptian cardiologists developed consensus statements on RAAS inhibitors for primary and secondary prevention of cardiovascular outcomes and stroke, using a modified three-step Delphi process.</p><p><strong>Results: </strong>The consensus statements highlight the importance of effective BP control and the role of RAAS blockade for prevention and management of various cardiovascular diseases. ACEis and ARBs differ in their mode of action and, thus, clinical effects. On the basis of available evidence, the consensus group recommended the following: ACEis should be considered as first choice (in preference to ARBs) to reduce the risk of MI, for primary prevention of HF, and for secondary prevention of stroke. ACEis and ARBs show equivalent efficacy for the primary prevention of stroke. Evidence also favors the preferential use of ACEis in patients with type 2 diabetes, for BP control, for the primary prevention of diabetic kidney disease, and to reduce the risk of major cardiovascular and renal outcomes. Treatment with an ACEi should be started within 24 h of ST segment elevation MI (and continued long term) in patients with HF, left ventricular systolic dysfunction, and/or diabetes. Angiotensin receptor/neprilysin inhibitors (ARNIs) are the first choice for patients with HF and reduced ejection fraction, with ACEis being the second choice in this group. ARBs are indicated as alternatives in patients who cannot tolerate ACEis. ACEis may be associated with cough development, but the incidence tends to be overestimated, and the risk can be reduced by use of a lipophilic ACEi or combining the ACEi with a calcium channel blocker.</p><p><strong>Conclusion: </strong>RAAS blockade is an essential component of hypertension therapy; however, the protective effects provided by ACEis are superior to those of ARBs. Therefore, an ACEi is indicated in almost all cases, unless not tolerated.</p>","PeriodicalId":9561,"journal":{"name":"Cardiology and Therapy","volume":" ","pages":"707-736"},"PeriodicalIF":2.7000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11607301/pdf/","citationCount":"0","resultStr":"{\"title\":\"ACE Inhibitors and Angiotensin Receptor Blockers for the Primary and Secondary Prevention of Cardiovascular Outcomes: Recommendations from the 2024 Egyptian Cardiology Expert Consensus in Collaboration with the CVREP Foundation.\",\"authors\":\"Mohamed Sobhy, Adel Eletriby, Hany Ragy, Hossam Kandil, Mohamed Ayman Saleh, Nabil Farag, Ramez Guindy, Ahmed Bendary, Ahmed Mohamed Elmahmoudy Nayel, Ahmed Shawky, Ayman Khairy, Ayman Mortada, Bassem Zarif, Haitham Badran, Hazem Khorshid, Kareem Mahmoud, Karim Said, Khaled Leon, Mahmoud Abdelsabour, Mazen Tawfik, Mohamed Aboel-Kassem F Abdelmegid, Mohamed Koriem, Mohamed Loutfi, Moheb Wadie, Mohamed Elnoamany, Mohamed Sadaka, Mohamed Seleem, Mohamed Zahran, Osama A Amin, Sameh Elkaffas, Sherif Ayad, Wael El Kilany, Walid Ammar, Waleed Elawady, Walid Elhammady, Yasser Abdelhady\",\"doi\":\"10.1007/s40119-024-00381-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The renin-angiotensin-aldosterone system (RAAS) plays a pivotal role in regulating blood pressure (BP), with dysregulation of RAAS resulting in hypertension and potentially heart failure (HF), myocardial infarction (MI), cardio-renal syndrome, and stroke. RAAS inhibitors, such as angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs), have advantages beyond BP control. However, differences between these two drug classes need to be considered when choosing a therapy for preventing cardiovascular events.</p><p><strong>Methods: </strong>A panel of 36 Egyptian cardiologists developed consensus statements on RAAS inhibitors for primary and secondary prevention of cardiovascular outcomes and stroke, using a modified three-step Delphi process.</p><p><strong>Results: </strong>The consensus statements highlight the importance of effective BP control and the role of RAAS blockade for prevention and management of various cardiovascular diseases. ACEis and ARBs differ in their mode of action and, thus, clinical effects. On the basis of available evidence, the consensus group recommended the following: ACEis should be considered as first choice (in preference to ARBs) to reduce the risk of MI, for primary prevention of HF, and for secondary prevention of stroke. ACEis and ARBs show equivalent efficacy for the primary prevention of stroke. Evidence also favors the preferential use of ACEis in patients with type 2 diabetes, for BP control, for the primary prevention of diabetic kidney disease, and to reduce the risk of major cardiovascular and renal outcomes. Treatment with an ACEi should be started within 24 h of ST segment elevation MI (and continued long term) in patients with HF, left ventricular systolic dysfunction, and/or diabetes. Angiotensin receptor/neprilysin inhibitors (ARNIs) are the first choice for patients with HF and reduced ejection fraction, with ACEis being the second choice in this group. ARBs are indicated as alternatives in patients who cannot tolerate ACEis. ACEis may be associated with cough development, but the incidence tends to be overestimated, and the risk can be reduced by use of a lipophilic ACEi or combining the ACEi with a calcium channel blocker.</p><p><strong>Conclusion: </strong>RAAS blockade is an essential component of hypertension therapy; however, the protective effects provided by ACEis are superior to those of ARBs. Therefore, an ACEi is indicated in almost all cases, unless not tolerated.</p>\",\"PeriodicalId\":9561,\"journal\":{\"name\":\"Cardiology and Therapy\",\"volume\":\" \",\"pages\":\"707-736\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11607301/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology and Therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s40119-024-00381-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology and Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40119-024-00381-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/25 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
ACE Inhibitors and Angiotensin Receptor Blockers for the Primary and Secondary Prevention of Cardiovascular Outcomes: Recommendations from the 2024 Egyptian Cardiology Expert Consensus in Collaboration with the CVREP Foundation.
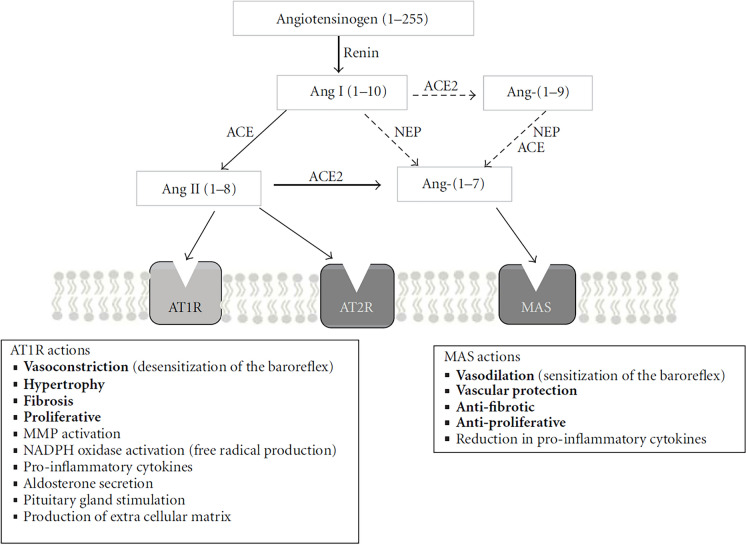
Introduction: The renin-angiotensin-aldosterone system (RAAS) plays a pivotal role in regulating blood pressure (BP), with dysregulation of RAAS resulting in hypertension and potentially heart failure (HF), myocardial infarction (MI), cardio-renal syndrome, and stroke. RAAS inhibitors, such as angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs), have advantages beyond BP control. However, differences between these two drug classes need to be considered when choosing a therapy for preventing cardiovascular events.
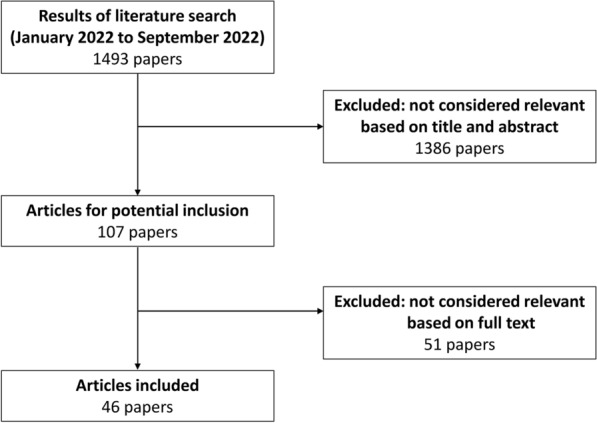
Methods: A panel of 36 Egyptian cardiologists developed consensus statements on RAAS inhibitors for primary and secondary prevention of cardiovascular outcomes and stroke, using a modified three-step Delphi process.
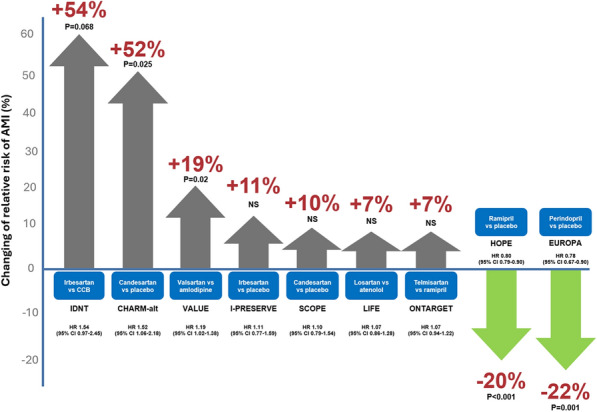
Results: The consensus statements highlight the importance of effective BP control and the role of RAAS blockade for prevention and management of various cardiovascular diseases. ACEis and ARBs differ in their mode of action and, thus, clinical effects. On the basis of available evidence, the consensus group recommended the following: ACEis should be considered as first choice (in preference to ARBs) to reduce the risk of MI, for primary prevention of HF, and for secondary prevention of stroke. ACEis and ARBs show equivalent efficacy for the primary prevention of stroke. Evidence also favors the preferential use of ACEis in patients with type 2 diabetes, for BP control, for the primary prevention of diabetic kidney disease, and to reduce the risk of major cardiovascular and renal outcomes. Treatment with an ACEi should be started within 24 h of ST segment elevation MI (and continued long term) in patients with HF, left ventricular systolic dysfunction, and/or diabetes. Angiotensin receptor/neprilysin inhibitors (ARNIs) are the first choice for patients with HF and reduced ejection fraction, with ACEis being the second choice in this group. ARBs are indicated as alternatives in patients who cannot tolerate ACEis. ACEis may be associated with cough development, but the incidence tends to be overestimated, and the risk can be reduced by use of a lipophilic ACEi or combining the ACEi with a calcium channel blocker.
Conclusion: RAAS blockade is an essential component of hypertension therapy; however, the protective effects provided by ACEis are superior to those of ARBs. Therefore, an ACEi is indicated in almost all cases, unless not tolerated.
期刊介绍:
Aims and Scope
Cardiology and Therapy is an international, open access, peer reviewed (single-blind), rapid-publication journal dedicated to the publication of high-quality clinical (all phases), observational, real-world, and health outcomes research around the discovery, development, and use of cardiovascular therapies and interventions, including devices. Studies relating to diagnosis and diagnostics, pharmacoeconomics, public health, quality of life, as well as patient care, management and education are also encouraged.
Areas of focus include, but are not limited to, ischaemic heart disease and acute cardiac care, myocardial, valvular, pericardial and congenital heart disease, vascular and pulmonary disease (including hypertension), arrhythmias, heart failure, non-invasive diagnostic techniques, and invasive and interventional cardiology as well as cardiovascular surgery.
The journal is of interest to a broad audience of pharmaceutical and healthcare professionals and publishes original research, reviews, case reports/case series, trial protocols and short communications such as commentaries and editorials. Cardiolology and Therapy will consider all scientifically sound research be it positive, confirmatory or negative data. Submissions are welcomed whether they relate to an international and/or a country-specific audience, something that is crucially important when researchers are trying to target more specific patient populations. This inclusive approach allows the journal to assist in the dissemination of quality research, which may be considered of insufficient interest by other journals.
Rapid Publication
The journal’s publication timelines aim for a rapid peer review of 2 weeks. If an article is accepted it will be published 3–4 weeks from acceptance. The rapid timelines are achieved through the combination of a dedicated in-house editorial team, who manage article workflow, and an extensive Editorial and Advisory Board who assist with peer review. This allows the journal to support the rapid dissemination of research, whilst still providing robust peer review. Combined with the journal’s open access model this allows for the rapid, efficient communication of the latest research and reviews, fostering the advancement of cardiovascular therapies.
Personal Service
The journal’s dedicated in-house editorial team offer a personal “concierge service” meaning authors will always have an editorial contact able to update them on the status of their manuscript. The editorial team check all manuscripts to ensure that articles conform to the most recent COPE, GPP and ICMJE publishing guidelines. This supports the publication of ethically sound and transparent research.
Digital Features and Plain Language Summaries
Cardiology and Therapy offers a range of additional features designed to increase the visibility, readership and educational value of the journal’s content. Each article is accompanied by key summary points, giving a time-efficient overview of the content to a wide readership. Articles may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand the scientific content and overall implications of the article. The journal also provides the option to include various types of digital features including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations. All additional features are peer reviewed to the same high standard as the article itself. If you consider that your paper would benefit from the inclusion of a digital feature, please let us know. Our editorial team are able to create high-quality slide decks and infographics in-house, and video abstracts through our partner Research Square, and would be happy to assist in any way we can. For further information about digital features, please contact the journal editor (see ‘Contact the Journal’ for email address), and see the ‘Guidelines for digital features and plain language summaries’ document under ‘Submission guidelines’.
For examples of digital features please visit our showcase page https://springerhealthcare.com/expertise/publishing-digital-features/
Publication Fees
Upon acceptance of your article for publication, authors will be required to pay the mandatory Rapid Service Fee of £3650/€4500/$5100. The journal will consider fee discounts for developing countries and this is decided on a case by case basis.
Open Access
All articles published by Cardiology and Therapy are published open access.
Peer Review Process
Upon submission, manuscripts are assessed by the editorial team to ensure they fit within the aims and scope of the journal and are also checked for plagiarism. All suitable submissions are then subject to a comprehensive single-blind peer review. Reviewers are selected based on their relevant expertise and publication history in the subject area. The journal has an extensive pool of editorial and advisory board members who have been selected to assist with peer review based on the afore-mentioned criteria.
At least two extensive reviews are required to make the editorial decision, with the exception of some article types such as Commentaries, Editorials and Letters which are generally reviewed by one member of the Editorial Board. Where reviewer recommendations are conflicted, the editorial board will be contacted for further advice and a presiding decision. Manuscripts are then either accepted, rejected or authors are required to make major or minor revisions (both reviewer comments and editorial comments may need to be addressed). Once a revised manuscript is re-submitted, it is assessed along with the responses to reviewer comments and if it has been adequately revised it will be accepted for publication. Accepted manuscripts are then copyedited and typeset by the production team before online publication. Appeals against decisions following peer review are considered on a case by case basis and should be sent to the journal editor.
Preprints
We encourage posting of preprints of primary research manuscripts on preprint servers, authors’ or institutional websites, and open communications between researchers whether on community preprint servers or preprint commenting platforms. Posting of preprints is not considered prior publication and will not jeopardize consideration in our journals. Authors should disclose details of preprint posting during the submission process or at any other point during consideration in one of our journals. Once the preprint is published, it is the author’s responsibility to ensure that the preprint record is updated with a publication reference, including the DOI and a URL link to the published version of the article on the journal website.
Copyright
Cardiology and Therapy is published under the Creative Commons Attribution-Noncommercial License, which allows users to read, copy, distribute, and make derivative works for non-commercial purposes from the material, as long as the author of the original work is cited. The author assigns the exclusive right to any commercial use of the article to Springer. For more information about the Creative Commons Attribution-Noncommercial License, click here: http://creativecommons.org/licenses/by-nc/4.0.
Contact
For more information about the journal, including pre-submission enquiries, please contact matthew.evans@springer.com

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


